
Stefan Kowal developed hoarseness two years ago. He had been seen twice by a laryngologist who told him he had a polyp on the right vocal cord and treated him with antibiotics, reassuring him it wasn’t cancer. His vocal quality fluctuated, such that at times he thought he was improving. Then he definitely became more hoarse. He now cannot yell or even be heard well with any background noise and he develops pain if he speaks very much.


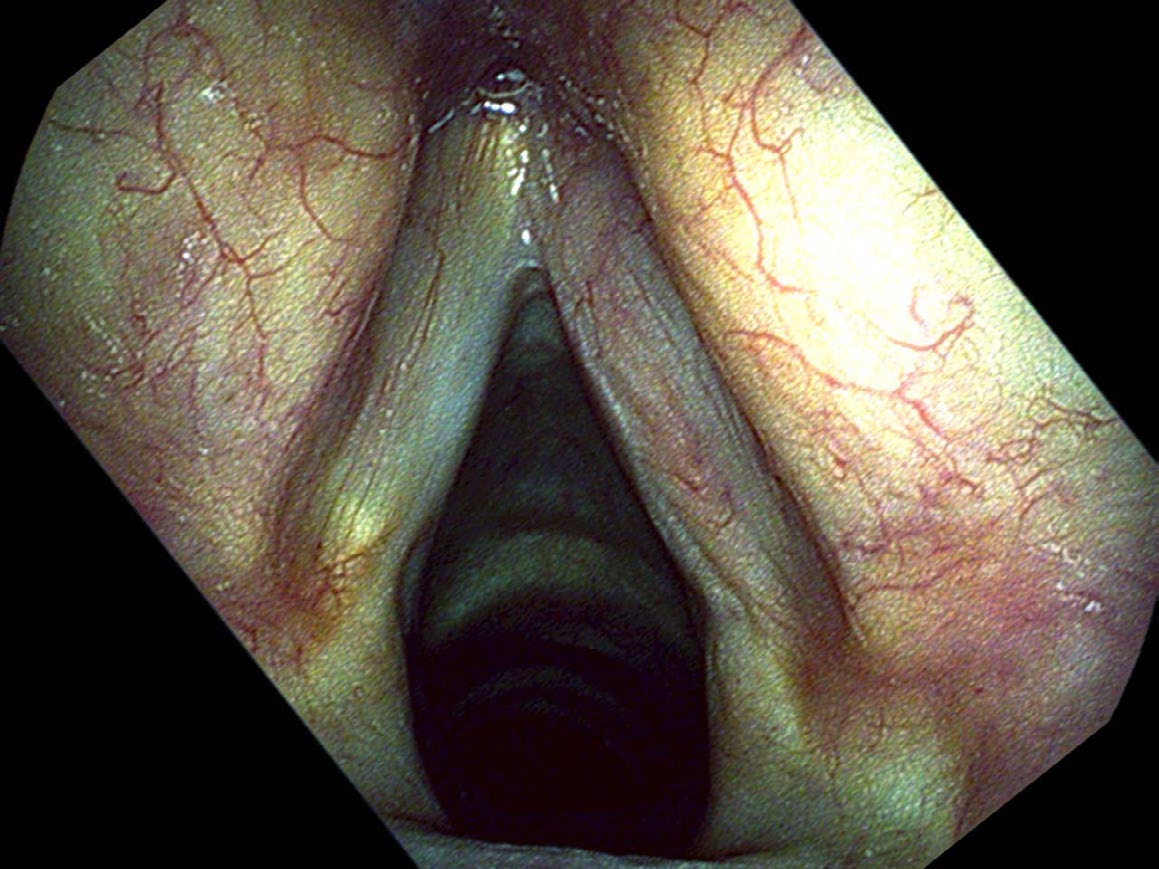
Physicians may over or underestimate the possibility of cancer. Some, who do not want their patients to be concerned, might underestimate the risk of cancer; others bring up the probability of cancer such that surgery seems like the smaller risk than the uncertainty of not knowing. In Mr. Kowal, I was in awe how such a large mass, covering the entire surface of one vocal cord, could be examined two years in a row and still be treated as a polyp. I suspect that equipment played a role, as the flexible fiberoptic scope found in many offices presents a blurry picture. There was no recording made of his prior exams; quite possibly the image in the eyes of the otolaryngologist was fleeting. Couple the problems of no recording and a blurry view with the possibility that the physician did not move the endoscope very close to the vocal cords and the delay in diagnosis is now understandable, even if not desirable.
Despite its rather extensive appearance, this cancer proved to be entirely on the surface and was peeled off of the right vocal cord with a CO₂ laser. One month after the surgery he still had a slightly elevated red area on the edge of the vocal cord. While this appeared to be a granuloma on my endoscopic examination, Mr. Kowal now had an elevated concern for any finding that might represent cancer. Since lesions with blood in them respond well to the office pulsed KTP laser, we treated this and the red lumps were gone by his next office visit.

For me, the reason that follow-up examinations are as important as the diagnosis is that I have cut closer to the cancer than many other surgeons. This leaves more normal vocal cord in place.
He returns to the clinic for frequent check-ups and the tumor has not recurred as of writing. Follow-up examinations are important in any patient with cancer. Because of the fear that the word cancer strikes in patients and physicians, there is a tendency to overtreat. Removing Mr. Kowal’s entire larynx with a total laryngectomy would have been equally effective treatment — more certainly it would have removed all of the cancer. However he would now be functioning without a voice box. When I removed Mr. Kowal’s tumor, I cut right on the interface of the tumor and his normal tissue. With regular, close examinations and with high-quality endoscopes, I believe that I will see any remnants or recurrences of the cancer early and can treat them appropriately while still very small.
This avoids the problem of surgical over-treatment that otherwise removes some normal vocal cord and makes the patient’s voice worse. It also avoids the problem of over-treatment with radiation therapy and chemotherapy. While radiation therapy is just as successful at treating small vocal cord cancers, normal tissue is exposed to the radiation and complications, such as a dry throat, are unnecessary and lifelong.
What you learned
- Squamous cell carcinoma of the vocal cord often presents with progressive hoarseness, pain with voice use, and an irregular, pebbled surface — but can be mistaken for a polyp without high-quality imaging.
- Recording endoscopic examinations is critical; a fleeting image seen through a blurry flexible scope can lead to serious diagnostic delays.
- A CO₂ laser can remove surface cancers precisely, leaving the underlying vocal cord intact — but precise cutting requires close margins and committed follow-up.
- Follow-up endoscopy is as important as the surgery itself: early detection of any recurrence allows targeted re-treatment without sacrificing additional vocal cord tissue.
- Total laryngectomy or radiation, while definitive, come with lifelong trade-offs; voice-sparing precision surgery with close surveillance can be equally effective for small surface cancers.