


A vocal polyp is more like a blister than a callus. Where a nodule is a thickening of the mucosa — the outer layer of the vocal cord — a polyp has a fluid collection beneath an otherwise normal outer layer. To the patient the vocal impairment may feel similar, but to a surgeon the distinction matters because treatment timing should be different. This chapter follows the unilateral hemorrhagic polyp — typically arising from a single vocal trauma. For the bilateral form driven by tobacco and talkativeness, see Smoker’s Polyps (Reinke’s Edema).
One-sided lesions are usually found in vocal non-overdoers. A single vocal indiscretion — a scream at a football game, a sudden forceful cough — is often the culprit.
The Unilateral Hemorrhagic Polyp
A Sudden Onset
“My voice has been rough for about eight months,” says Charles Earl Osterman, who manages a large medical group. “It used to be low and now it is lower and rough. I have also lost my upper range.” He rates himself a 4 on the talkativeness scale — not a vocal overdoer by nature — but in meetings he projects to fill a room. His voice was fine until one morning he woke up hoarse after an especially long day.
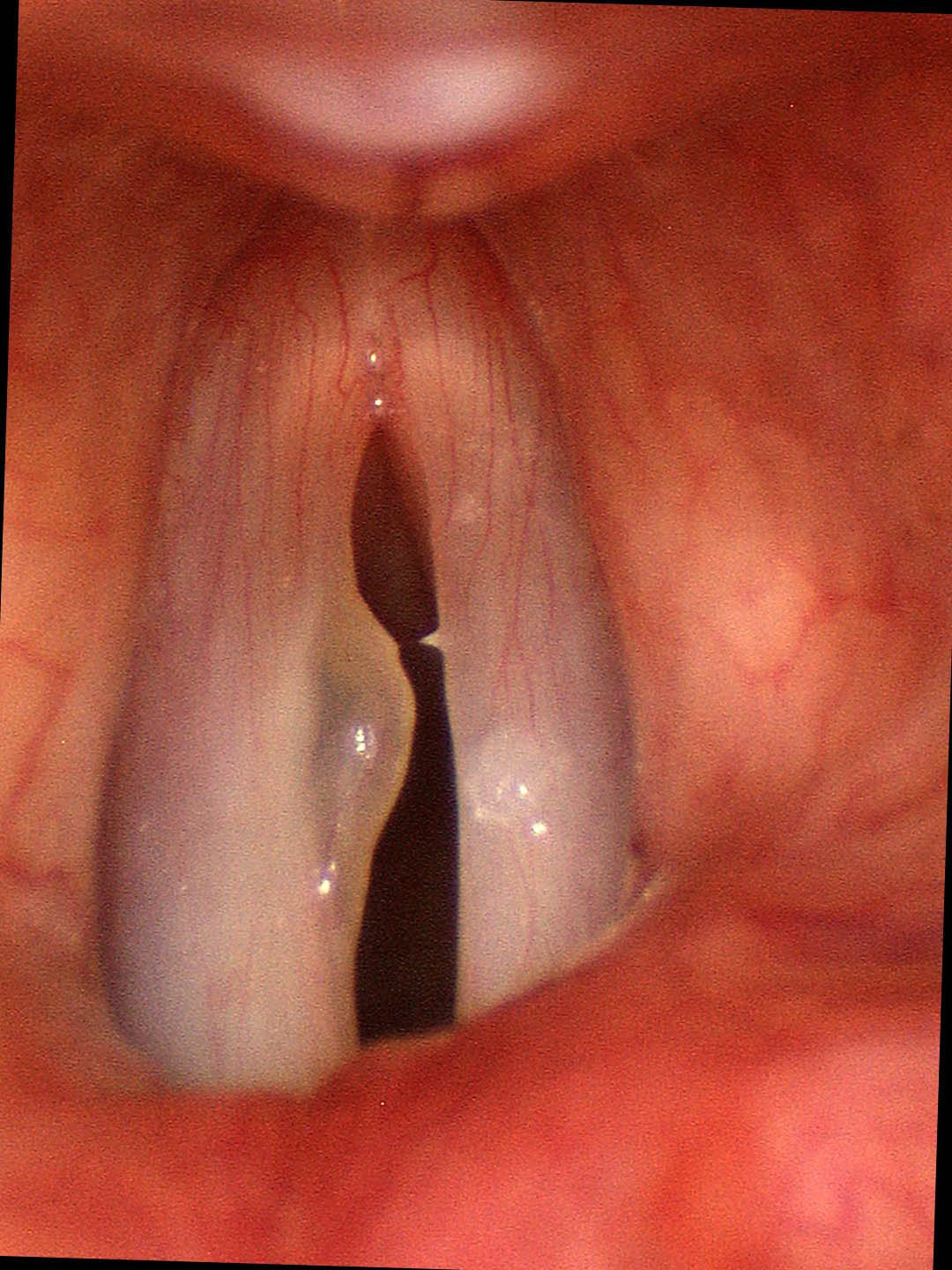
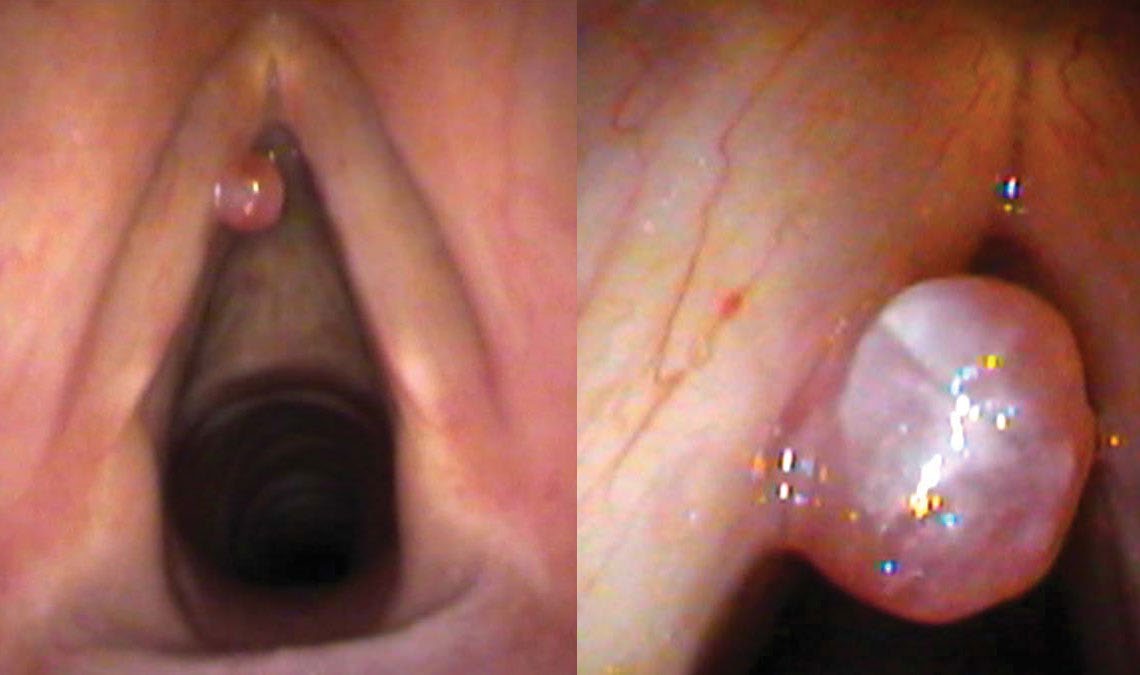
On the swelling test there is an onset delay starting at a consistent note in his mid range. I hear the roughness and the air leak in his voice when he speaks and these qualities are even more evident on swelling testing. On endoscopy there is a one-sided, spherical swelling on the vibrating edge of the left vocal cord — red in color and hemispherical. There is a smaller reactive swelling on the right side, induced by the polyp on the left striking the right cord hundreds of thousands of times in the same spot.
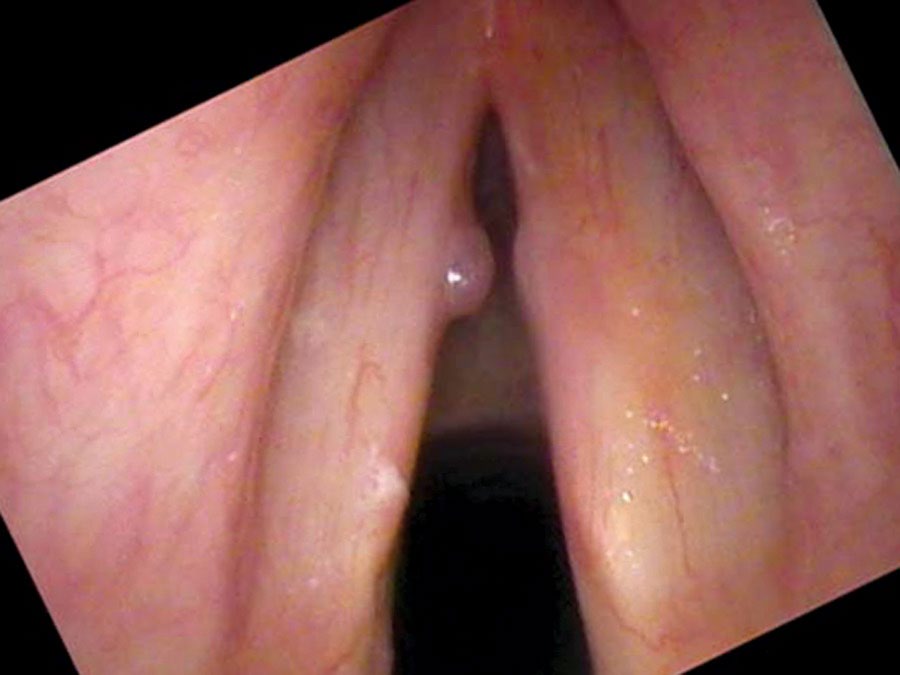
There is a large and slightly tortuous blood vessel crossing the surface of the vocal cord and leading to this polyp. The polyp flips up and out of the way when he speaks at a low pitch. If asked to raise his pitch, the polyp stands out and prevents him from making a higher pitch. Since he doesn’t sing, the loss of high notes bothered him less than it might have — which explains why he tolerated such a large swelling for months before seeking treatment.
Cause and Mechanism
One-sided polyps — with a feeding vessel or without — are commonly caused by a single vocal indiscretion: a scream at a football game, a sudden forceful cough, or a single vocal trauma. A loud, forceful slamming of the vocal cords together causes a rupture of a blood vessel. Blood beneath the mucosa creates a raised area. In the case of a clear polyp, the blood has reabsorbed but a proteinaceous, mucoid fluid remains. In the case of a broken blood vessel, it heals with a thin wall, effectively creating a weak aneurysm on the vibrating edge — repeatedly exposed to the trauma of phonation. That blood vessel often persists in a dilated form and may keep breaking and re-filling the polyp with blood.
The voice may worsen temporarily with vocal use because the polyp, flipping around on the edge of the cord centrifugally, fills with blood and temporarily enlarges. With voice rest the blood drains from the polyp and the voice returns to its baseline level of hoarseness — a telltale fluctuating pattern.
Treatment and Recurrence
Since there is no chronic vocal behavior problem driving a one-sided lesion, the primary approach is surgery: excise the lesion and cauterize or interrupt the feeding blood vessel. Voice behavior modification is not the starting point, because there is no bad habit to modify. After surgery Charles Earl Osterman improved and returned to regular work. Three months later, with a cough, he developed a hoarse voice again — the hemorrhagic polyp was back, with a new feeding vessel.
The polyp was removed a second time in the office by cutting it at the base and cauterizing the feeding blood vessel with a laser. It has not recurred since. The lesson: if an enlarged vessel is present on the vibrating edge of the vocal cord, it will be more subject to breakage from vocal trauma. The offending vessel must be addressed — not just the polyp it feeds.
What You Learned
- A polyp is like a blister — a fluid collection beneath the mucosa — while a nodule is like a callus, a thickening of the mucosa itself. The distinction guides treatment timing.
- Unilateral hemorrhagic polyps typically arise from a single vocal indiscretion and are found even in non-overdoers. Surgery is the primary treatment because there is no behavioral pattern to modify.
- A recurrent polyp often means an incompletely cauterized feeding blood vessel. The vessel — not just the polyp — must be addressed to prevent recurrence.