
Sound production begins when the vocal cords move to the middle and come into alignment parallel to each other. Air is passed through the vocal cords from the windpipe and they start to vibrate, creating sound. At a comfortable speaking pitch they open and close perhaps 100 times per second in a typical male voice and perhaps 200 times per second for a typical female. With each vibration the vocal cords collide with each other, most forcefully in the middle of the vocal cord. It would not take much to have over a million collisions per day — and yet, the vocal cords can generally handle a lot of vibrations. At some point, though, the cords collide often enough and strongly enough that the mucosa begins to react.
You cannot develop symmetric or nearly symmetric swellings in the middle of the vocal cord other than through vocal overuse.
The Callus Analogy
Just as the skin of the hands reacts to extensive use by forming blisters and calluses, the same is true for the vocal cords. The mucosa can thicken like a callus, or fluid may accumulate beneath it in its central portion, like a blister. These are the lesions referred to as vocal nodules and vocal polyps — also called singer’s nodules in lay terms. They are no more harmful to the body than a callus on the hand; they are not growths. However, they do have a significant impact on the voice.
Why doesn’t everyone get them? Some people talk non-stop with seemingly few side effects. Others will lose their soft vocal range after one evening in a loud bar. Whether due to technique, genetic predisposition, or some other factor, some people are clearly more susceptible than others to vocal overuse. Three things probably play a role in their development: quantity of vocal use (talkativeness), intensity of vocal use (loudness), and technique of vocal use. Quantity has the highest correlation, while volume plays the second most important role.
How Swellings Impair the Voice
Since swellings occur in the middle of the vocal cord, they cause several predictable effects. They have mass, so the voice feels heavier — the pitch actually lowers as the mass of the cord increases. Because the thickening develops slowly over months or years, the patient may not notice this gradual deepening. In cases where a thickening is removed by surgery, the patient will often notice the abrupt lightness and suppleness of the voice immediately, because the change is so sudden.
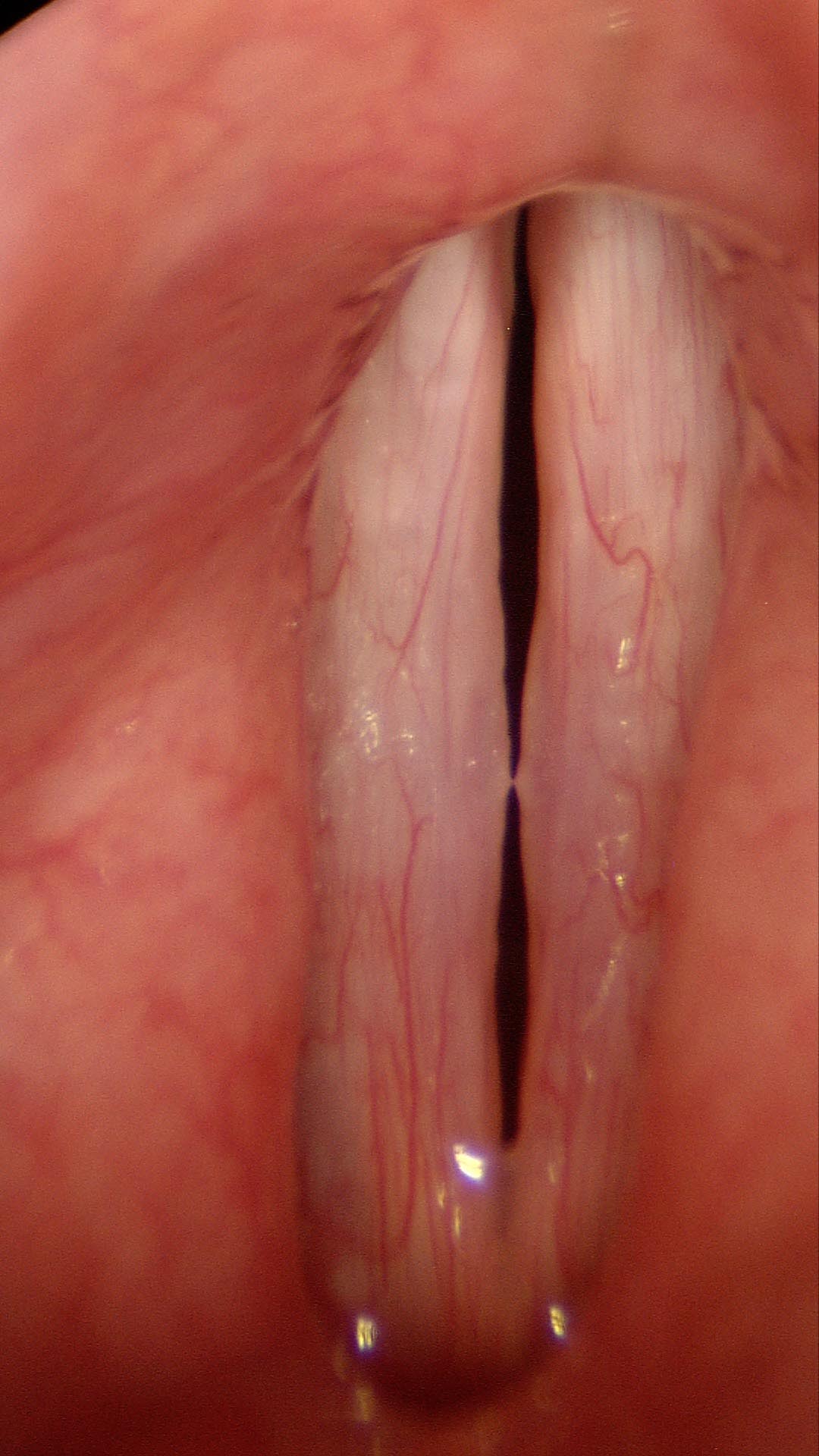
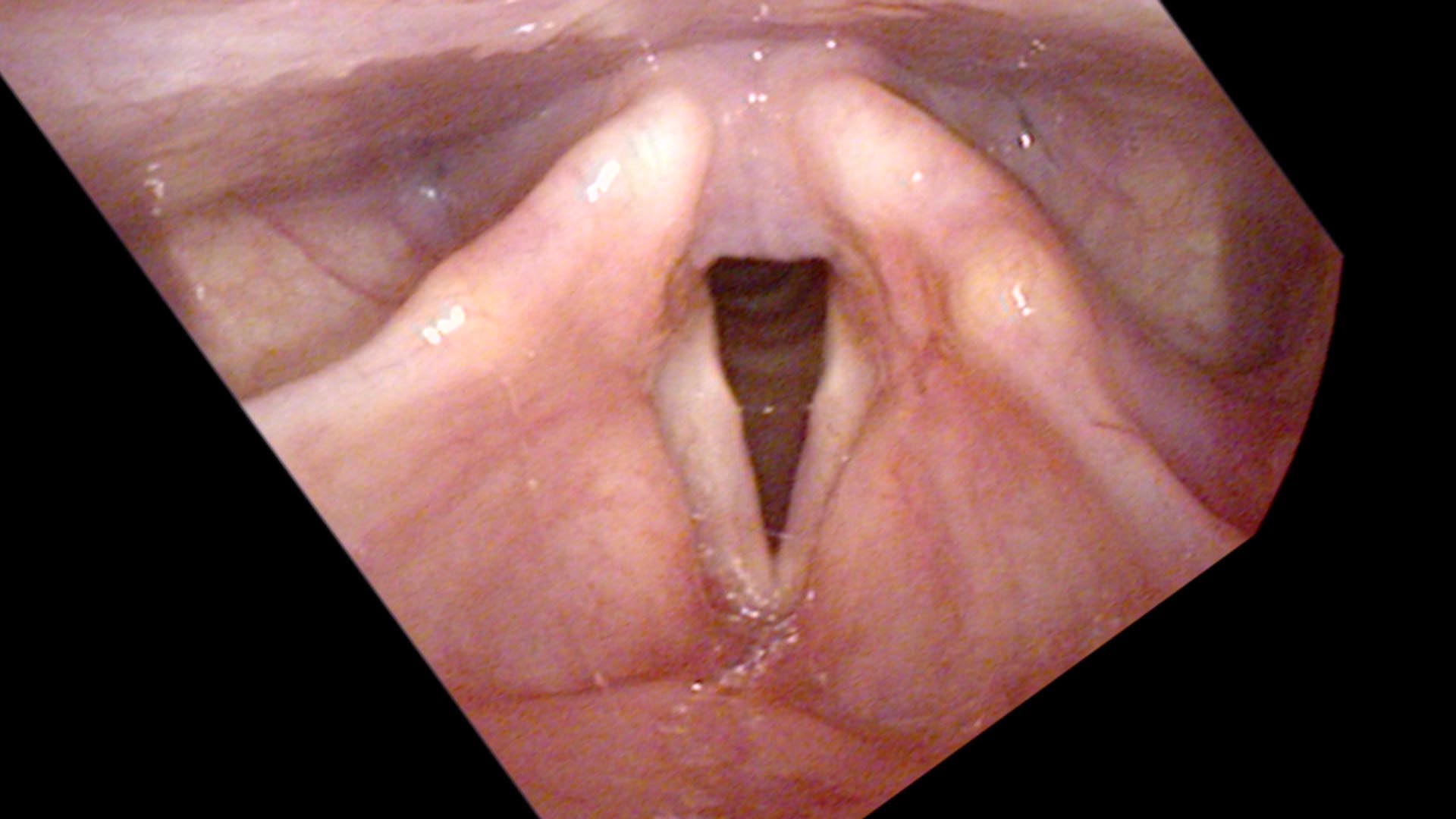
When the vocal cords are brought into a closed position, the opposing swellings touch one another before the cords completely line up, creating a gap in front of and behind the swellings through which air leaks. Because they touch, there is a dampening of vibrations that prevents soft phonation. Think of trying to play the violin while someone lightly touches the string: it requires more force with the bow to set the string vibrating. The lungs must push more air to start vibrations, and there will be audible onset delays at the start of soft phonation.
With time, the individual develops compensation — holding the vocal cords slightly apart to keep the bumps from touching. This requires simultaneous activation of the LCA muscle (which brings the cords together) and the PCA muscle (which keeps them apart). Two opposing muscles competing against one another produce vocal discomfort, pain, and fatigue.

Diagnosing Vocal Nodules
As pitch is raised the vocal cords stretch, straighten, and tighten. The tightening pushes the swelling to protrude more. The patient will reach a pitch where the swellings protrude just enough to touch — and if the volume is soft, that touching prevents vibrations from starting. There will be an onset delay or no phonation at all. This cut-off happens on a very consistent note, making it a reliable diagnostic sign.
I ask the patient to sing the first line of “Happy Birthday to You.” Between the word “day” and “to” there is a jump of three half-steps. As the patient ascends the scale softly, there will be one pitch at which the word “to” fails to come out — where the swellings touch and dampen vibration. Below this note the swellings are apart and do not impair initiation of sound. Above it, the bumps touch tightly enough to divide the vibrating cord into two segments, just like touching a guitar string in the middle — producing a sudden pitch jump or diplophonia (double pitch).


Three Kinds of Vocal Overdoers
Benign mucosal swellings almost uniformly appear in vocal overdoers — people who innately enjoy talking and rate themselves a 5, 6, or 7 on a talkativeness scale of 1 to 7. Within that group, three clinical patterns recur.
The Talkative Professional
“My voice gets scratchy by late afternoon,” says Mrs. Chatterly, a teacher. “By the time I get home it is nearly gone. After resting over the weekend it is back to normal, but within a day of teaching it starts to deteriorate again.” She rates herself a 7 on the talkativeness scale — “I have always loved to talk” — and speaks loudly in a classroom all day. She has been self-treating with throat lozenges, honey in her tea, and humidifiers for months.
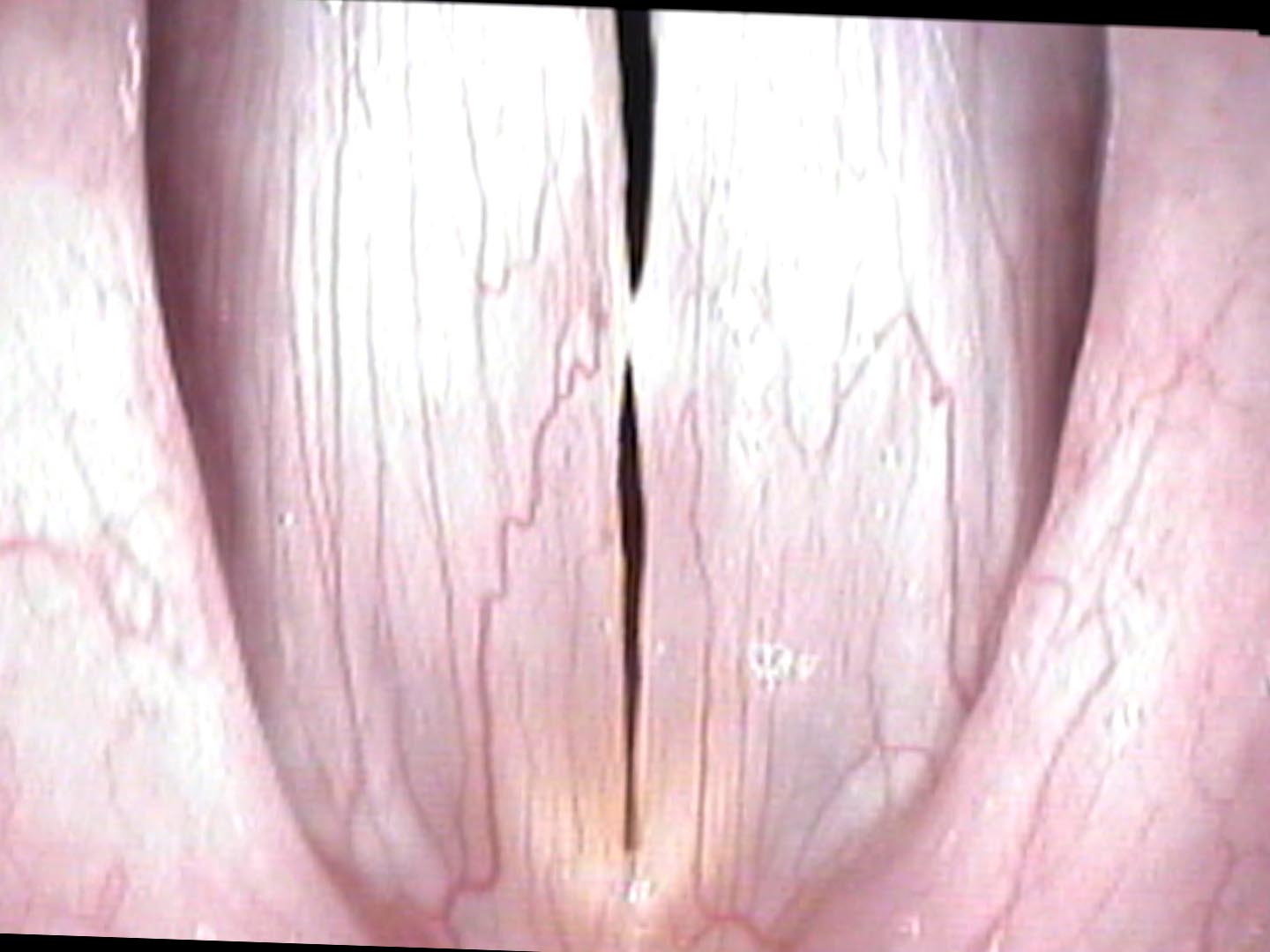
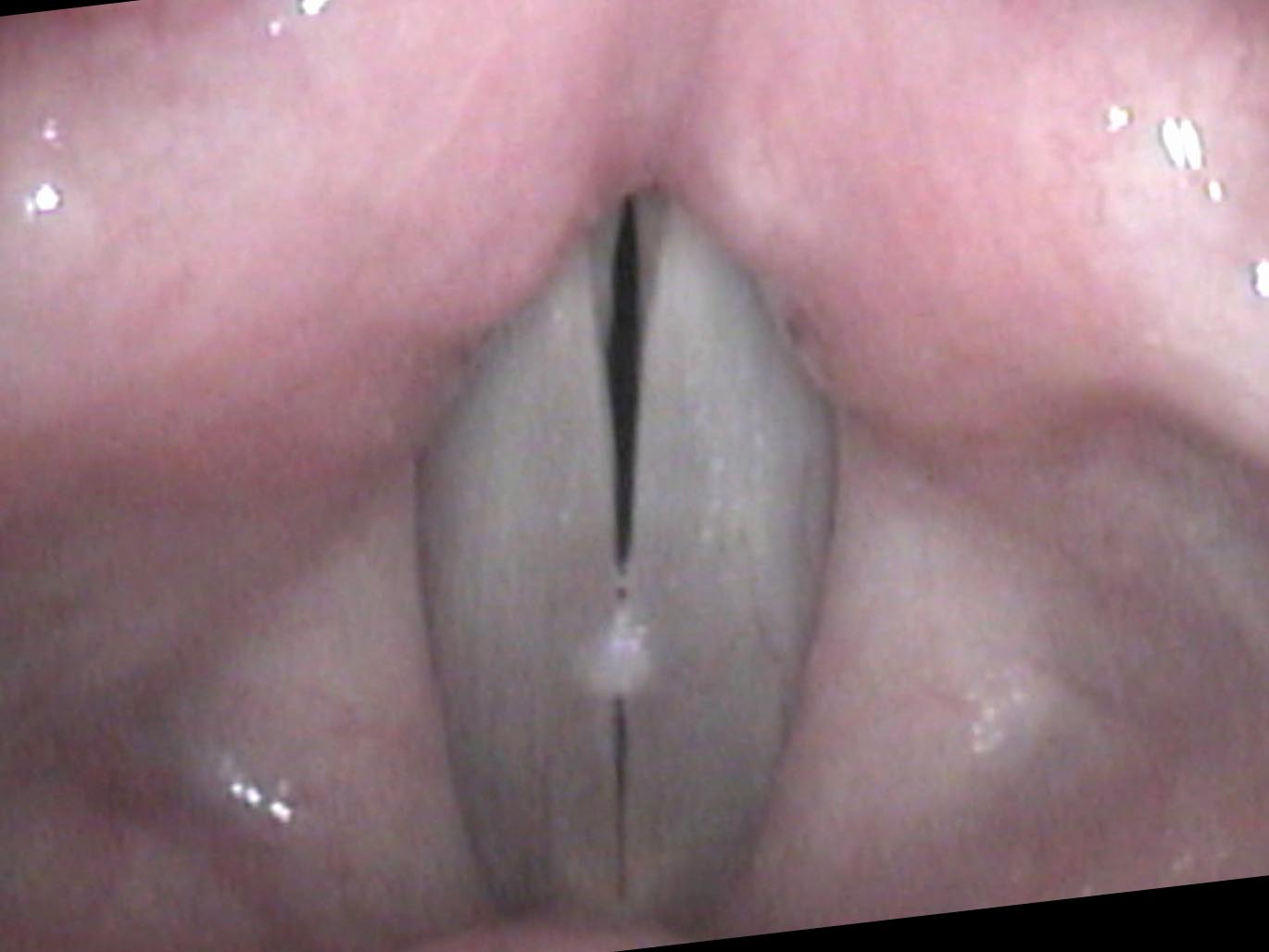
On vocal capabilities testing, her speaking pitch is lower than average for a woman her age. The swelling test reveals an onset delay on a specific note, consistent on repeated trials. On endoscopy, there is a bilateral swelling in the center of her vocal cords with a small air leak behind them. Two vocal cord swellings from overuse. Her lesson plan has been her downfall — or rather, her love of teaching has been.
The Explosive Yeller
“My voice has been hoarse and deep for the past four months,” says Johnny Quicktemper, a construction foreman. “My wife says it sounds like I have a cold all the time.” He rates himself only a 4 on the talkativeness scale — not innately chatty — but his job involves yelling: instructions across a noisy site, reprimands to workers, commands over machinery. Volume drives his swellings as much as quantity.
The vocal capabilities reveal a low speaking pitch and a consistent onset delay on swelling testing. On endoscopy there are bilateral nodules with ectatic blood vessels nearby — evidence of repeated micro-hemorrhage into the cord over time. His wife’s observation was correct: he sounds hoarse all the time, and the swellings will persist as long as he continues yelling.
The Trained Singer
“I can’t sing the high soft notes anymore,” says Amour T. Cher, a voice teacher who performs semi-professionally. “They were always my best notes.” She has been training for fifteen years and recently started a second studio. Between teaching, rehearsals, and performances her vocal use has quietly doubled — though she has not changed her warmup or cool-down routine.
Classical singers have unusually precise awareness of their voices, which is why they are often the first to detect even small swellings. On swelling testing, the onset delay falls squarely in her professional singing range — the pitches she needs most. On endoscopy, bilateral swellings are present, modest in size but strategically positioned to silence exactly the pianissimo high notes her students expect her to demonstrate.

A nodule represents a thickening of the mucosa — the outer layer of the vocal cord. It is analogous to a callus on the hand.
Treatment: Voice Therapy First, Surgery Last
The cornerstone of treatment for bilateral vocal nodules is voice therapy. Because the overuse created the swellings, reducing overuse can resolve them. Vocal nodules in a consistent overdoer tend to reappear quickly after surgical excision unless the vocal behavior is addressed first. A vocal overdoer — someone who rates 6 or 7 on the talkativeness scale — genuinely believes that non-stop talking all day is normal behavior. Voice therapy gives the patient insight into how much they are really using their voice and provides strategies to reduce the impact of each vibration.
If behavioral management succeeds in reducing overuse yet the lesion persists after several months, surgery becomes an option. After removal of swellings, the voice typically becomes very easy and effortless to use — which proves to be a license to talk for the vocal overdoer. A good voice therapist can continue working after surgery to modify vocal behavior and prevent recurrence. Muscle memory also plays a role: if the swellings have been present for a long time, the patient may continue to hold the cords apart out of habit even after surgery, and a therapist can retrain the pattern of onset.
What You Learned
- Vocal nodules are callus-like thickenings that form in the center of the vibrating vocal cord — always from overuse, never from underuse.
- They appear almost exclusively in vocal overdoers: people who rate 5–7 on a talkativeness scale, especially those who also speak loudly.
- The swellings create predictable, testable effects: lower speaking pitch, onset delays on soft phonation at a consistent note, air leak, and diplophonia with larger lesions.
- Bilateral, symmetric mid-cord swellings mean overuse. One-sided swellings more often indicate a vocal indiscretion or a different type of lesion (polyp).
- Voice therapy is the first-line treatment — it reduces recurrence by addressing the underlying behavior. Surgery is reserved for lesions that persist after behavioral change.