
“My ENT doc sent me here,” Sam Sales notes. “I went in to see him because of a pain in my neck on the right side about six months ago. He looked with a scope and found a growth on my voice box. He took it off and it was benign. However, on a check-up it came back, so he put me on an antacid. I didn’t have any heartburn, but he said silent reflux can come up and burn my voice box and cause a growth.” Sam uses his voice all day as a consultant. “My voice fades out by the end of the day. It usually recovers by the next day.”
“I was involved in an accident three years ago and had a tube put down my throat,” he adds. “That may have been the cause of this.”
“Did your voice change when they took the tube out three years ago?”
“No, it was the same. My voice only began changing about six months ago.”
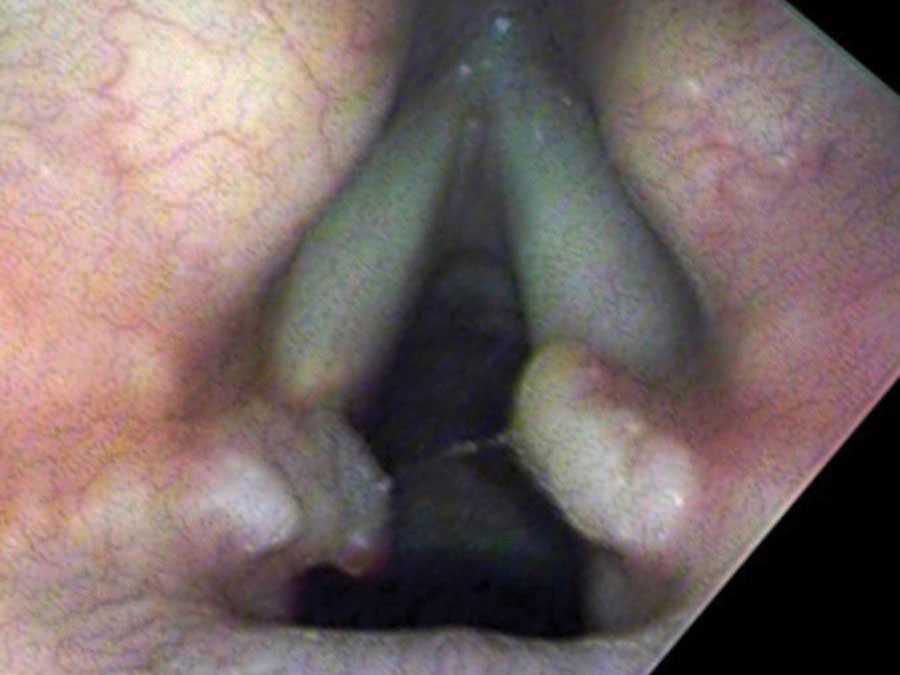
On endoscopy, there is a surprisingly large lump on the right vocal process — a yellow ball of tissue sitting just above an ulcerated groove in the cartilage.
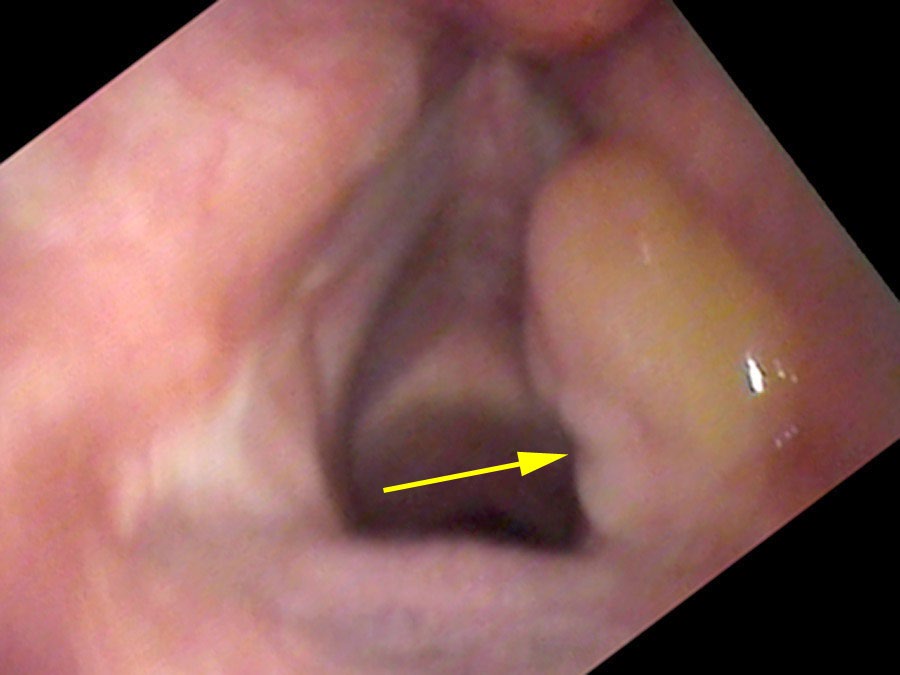
It really isn’t a growth. It is a collection of blood vessels wound into a little ball — what surgeons call “proud flesh” when it forms on the outside of the body.
What Is a Granuloma?
There is one particular type of vocal cord lesion that may start with a temporary pain and is located at the back of the larynx — most commonly on the cartilage called the vocal process of the arytenoid, right at the end of the vibrating portion of the vocal cord. It is not really a growth. Rather it is a collection of blood vessels wound into a little ball — called proud flesh when it forms on the outside of the body. When something traumatizes the mucosa, eroding through it and exposing the cartilage, an ulcer forms. Then granulation tissue heaps up around the traumatized point as a reaction to an open wound exposed to the bacteria of the mouth and throat.
The open ulcer often initially causes pain. That pain can masquerade as ear pain — because the tenth cranial nerve supplies both the larynx and the ear. It is not uncommon for individuals to experience pain shooting up into the ear on the affected side. An ear doctor should always scope the vocal cords when there is unexplained ear pain for exactly this reason. Pain from a granuloma ulcer is one-sided and can be quite sharp. It is different from muscle tension pain, which tends to be diffuse, achy, and located in the midline neck.
What Caused the Trauma?
Intubation Injury
An example of a single injury that can cause a granuloma is from an endotracheal intubation. During surgery under general anesthesia the plastic tube put through the larynx tends to put the most pressure on the vocal processes — bony prominences that stand prominent at the narrowing of the airway. After the tube is removed, an ulcer often forms on or near the vocal process. While these ulcers are thought to be rare, I suspect they are more common than believed. I have examined patients endoscopically every day after a general anesthetic and found ulcers to be rather common — yet they heal within days without any residual problem in most cases.
Sam’s granuloma was unlikely to be from his intubation three years earlier — his voice hadn’t changed at all until six months ago. When granulomas come from a single intubation injury, they typically do not recur, because the trauma is not repeating. Sam’s recurrence after surgical removal pointed to an ongoing cause.
Chronic Trauma: Bowing and Compensation
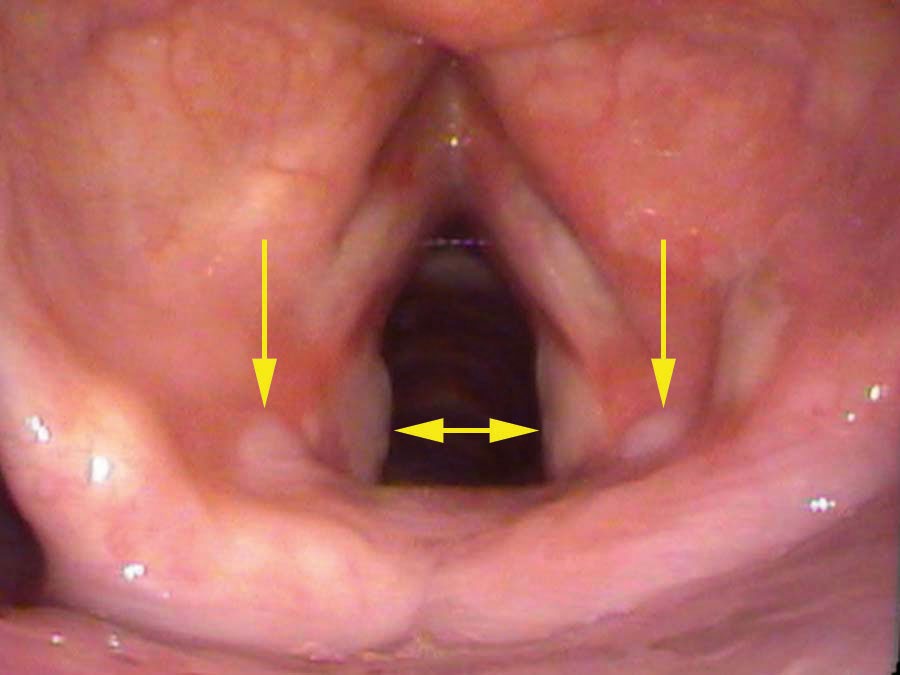
Sam’s more likely cause is compensation for vocal cord bowing. His vocal cords are visibly thin — a thyroarytenoid muscle that has atrophied or is weakened causes the cord to bow. When he closes his vocal cords to speak, the bowed cords fail to seal cleanly, so he squeezes harder to compensate. That harder squeeze drives the vocal processes — small cartilage knobs at the back of the cords — into each other with greater force than normal. Over time the mucosa over the cartilage erodes and an ulcer forms; granulation tissue follows.
Other chronic trauma scenarios include: a prolonged cough (vocal processes slamming together repeatedly at high force), a severe vocal overuser who speaks aggressively and loudly, or an older patient with vocal cord atrophy requiring compensation. The shared mechanism is always the same: forceful and frequent striking of the vocal processes against each other, erosion of the overlying mucosa, and the formation of an ulcer.
The Life Cycle of a Granuloma
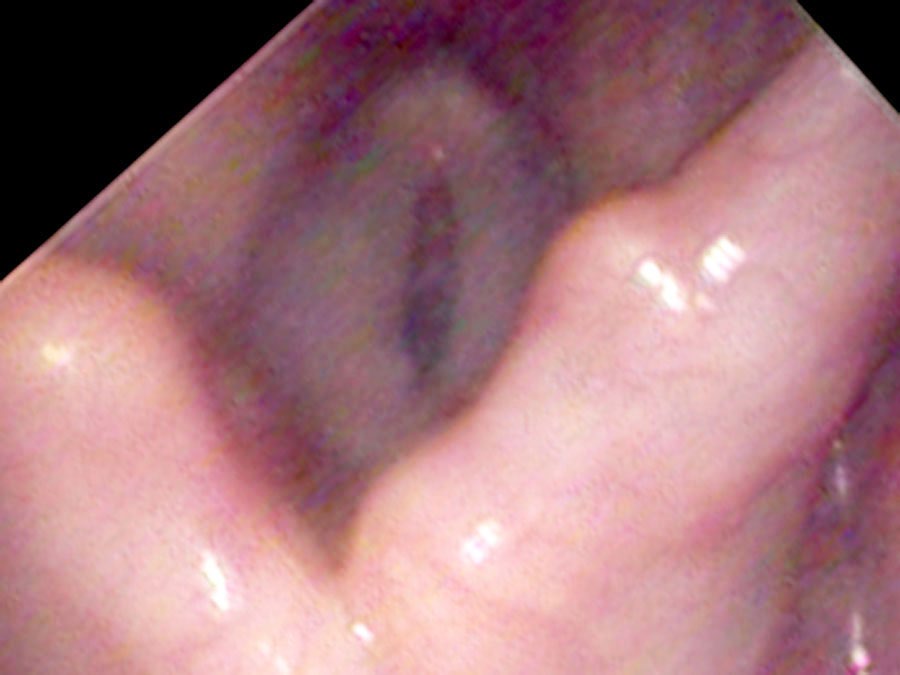
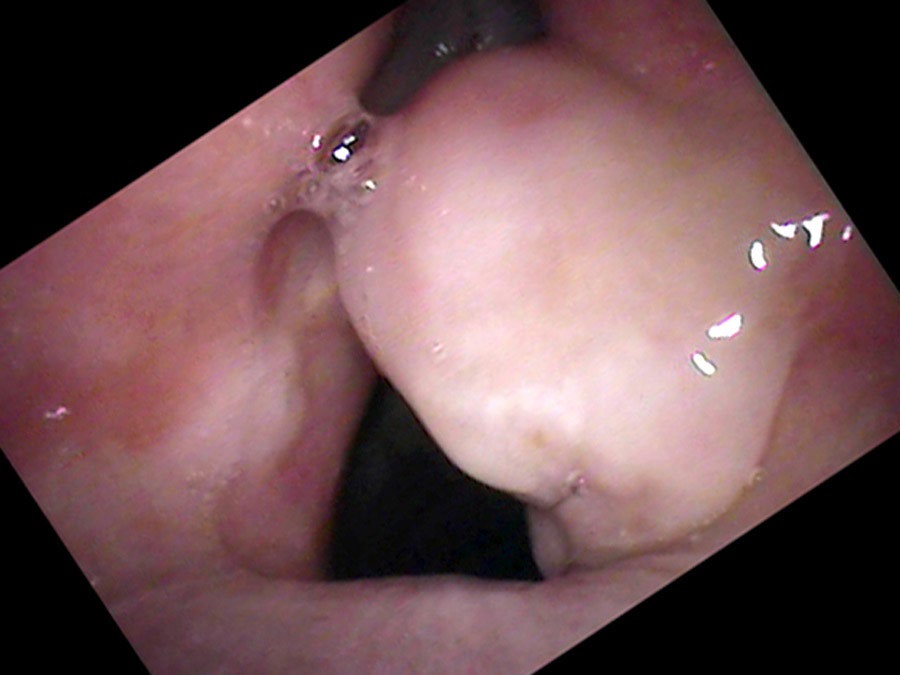
From injury to resolution, granulomas follow a predictable evolution. New ulcers from overuse initially split into two parts where the opposite vocal process rests in a groove during closure. Gradually, granulation tissue heaps up around the traumatized point, forming a mass. In the middle of their lifespan granulomas become yellow or red and round. Later the mass tends to harden, become white and spherical, and the base narrows to a stalk. At this stage the granuloma may flip up out of the way during phonation and no longer impairs closure — so vocal capabilities testing can return to normal even while the granuloma is still present.
Eventually the granuloma hangs from a thinner and thinner stalk before it falls off or is coughed off. Sam came back a year later: “About two weeks ago I was yelling at a baseball game. I coughed out something that looked like a BB and felt a sharp pain on the left side of my throat.” The self-decapitation of the granuloma is a common and self-limiting event — though as long as the underlying cause persists, recurrence is expected.
Treatment
The treatment of granulomas must address the underlying cause, not just the granuloma itself. If the granuloma is removed surgically while the cause is not addressed, each surgery opens a fresh wound at the base that can be re-traumatized immediately, restarting the cycle. At a minimum, voice rest after surgery until the mucosa has healed reduces the frequency of recurrence.
In Sam’s case, the strategy combined two injections delivered in the office: a steroid (triamcinolone) injected directly into the granuloma to reduce its size, and botulinum toxin injected into the LCA muscle to weaken closure of the vocal cords — reducing the impact of the vocal processes against each other. When he returned two months later, the granuloma had shrunk rather than being coughed out as often happens.

The longer-term solution for Sam’s bowing is augmentation: placing implants (medialization) into the vocal cords to bulk them up artificially, so he no longer needs to close them with such force. Until the bowing is corrected, ulcers and granulomas will recur. If he could cease speaking entirely, they would resolve — but that is not a practical solution for a consultant who uses his voice all day.
The reason for Sam’s granuloma was a traumatic wound of the larynx that created an ulcer. The answer to what caused the wound determines the treatment.
What You Learned
- A granuloma is not a true growth — it is granulation tissue (proud flesh) that forms in response to an ulcer over exposed cartilage at the back of the larynx.
- The pain from a granuloma ulcer is often felt as ear pain on the same side — a referred pain via the tenth cranial nerve that should prompt examination of the larynx.
- Granulomas can result from a single intubation injury (typically self-resolving) or from chronic trauma — repeated forceful striking of the vocal processes from bowing, coughing, or aggressive vocal use.
- Surgery without addressing the underlying cause leads to recurrence. The goal is to eliminate the mechanical trauma — through voice rest, botulinum toxin, or vocal cord augmentation.
- Granulomas follow a predictable life cycle from ulcer → active granuloma → mature stalked granuloma → self-decapitation. The process runs several weeks to several months.