
Tiny capillaries run the length of the vocal cords in parallel with the vibrating edge. Under normal conditions they are barely visible. When a vocal cord is traumatized — by chronic over-talking, high-volume speaking, screaming, a forceful cough, or aggressive singing — blood vessels may break and blood seeps out into the cord, producing a beet-red vocal cord after an acute injury. As the blood absorbs over several weeks, the cord turns gradually more yellow before all the hemoglobin is reabsorbed.
Whenever I see unusual capillaries — taking a tortuous path or running at odd angles to the length of the vocal cord — I suspect a prior history of severe vocal overuse. They form a historical record written in the cord itself.
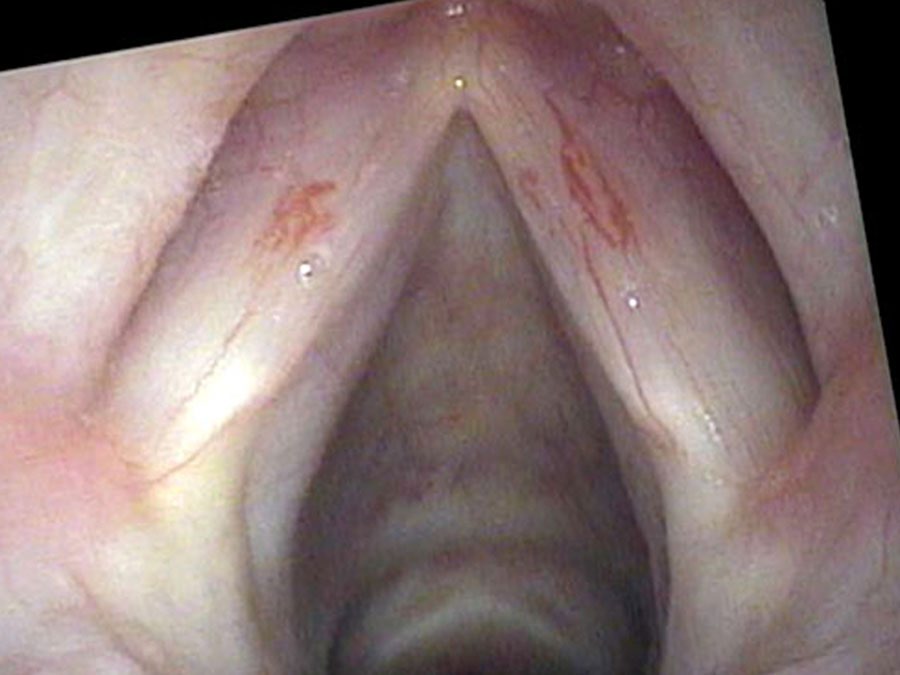
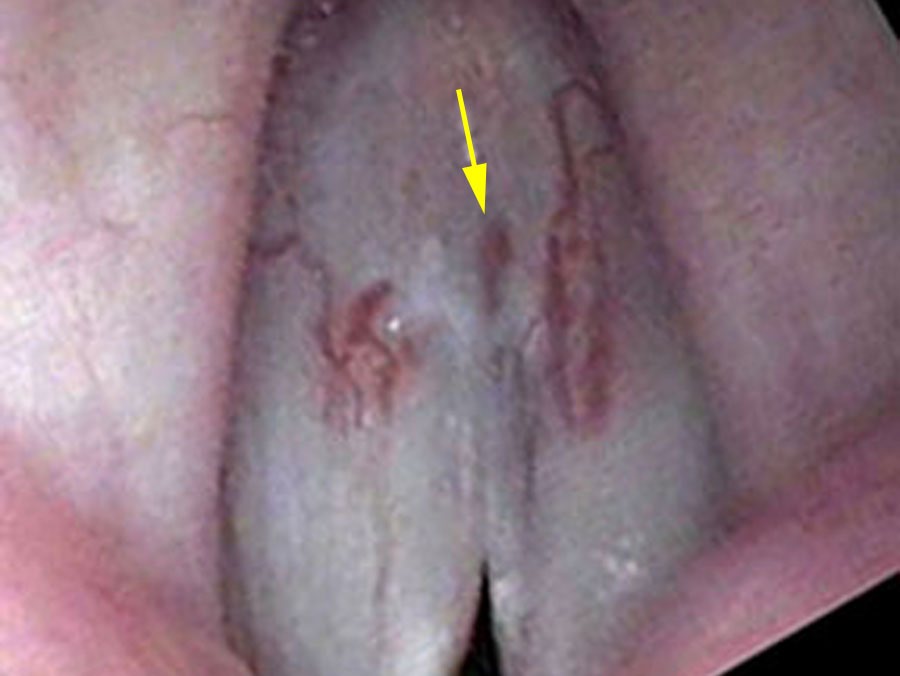
Tortuous and Dilated Capillaries
The broken blood vessel, as it heals, will often take a more tortuous path or remain dilated, perhaps because the injured walls of the vessel are thinner and weaker. So whenever I see unusual capillaries — capillaries taking a tortuous path, capillaries running at odd angles across rather than along the length of the cord — I suspect a prior history of severe vocal overuse. These unusual vessels are often located in the mid-portion of the vocal cord where the most trauma occurs. They are not dangerous in this location, but they are a record of the voice’s past.
Capillaries on the Vibratory Edge
When capillaries are located on the edge of the vocal cord, the situation is more consequential. As the vocal cords vibrate rapidly these vessels become filled with blood and swell, impairing the vibrations of the vocal cord and the person’s voice. In this location they are also more likely to rupture with further vocal use. An edge capillary can enter a polyp — where it becomes the “feeding vessel” — or it can sit directly on the vibratory margin, dilating with each phonation cycle and impeding complete closure.
During stroboscopy the vibrating edge of the vocal cord everts — rotates outward — with each vibration cycle, and this momentarily reveals capillaries that are otherwise hidden on the underside of the cord’s margin. A careful examiner watching slow-motion stroboscopy can identify dilated edge vessels that would be invisible at normal frame rates.
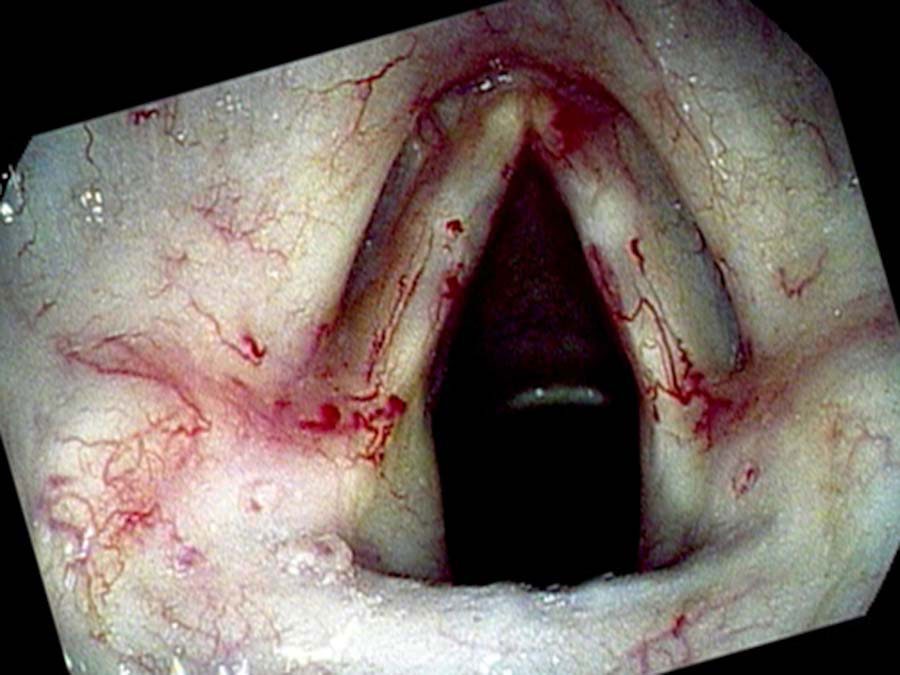
Radiation-Induced Telangiectasias
A second cause of vascular ectasia is radiation therapy. After radiation is used to treat vocal cord cancer, very tortuous capillaries grow gradually over several years throughout the radiation field. They resemble the roots you might see as you lift a plant out of a pot — dense, irregular, and multidirectional. As long as these capillaries are not on the vibrating edge of the vocal cord they generally do not interfere with sound production. When they form on the edge, however, they may dilate with vocal use and impair the closure of the vocal cords, producing a husky quality and air leak.
Clinical Significance
Ectatic vessels are often incidental findings noted during a complete laryngeal examination and do not necessarily require treatment. Their significance depends entirely on location: mid-cord tortuous capillaries are a historical marker, while edge vessels are a source of active impairment and re-bleeding risk. When edge capillaries are responsible for recurrent hemorrhagic polyps, they can be targeted with vascular-selective lasers such as the pulsed KTP laser, which delivers energy absorbed specifically by hemoglobin while sparing the surrounding mucosa.
What You Learned
- Vocal cord capillaries run parallel to the edge of the cord. Trauma — overuse, coughing, radiation — can rupture them, and the healed vessels often become tortuous or permanently dilated.
- Tortuous capillaries in the mid-cord are a historical record of overuse. They are generally not clinically significant in that location.
- Capillaries on the vibratory edge swell with each phonation cycle, impair closure, and are prone to rupture — they are the “feeding vessels” of hemorrhagic polyps.
- Radiation therapy produces its own distinctive pattern of vascular ectasia that can appear years after treatment. Edge involvement causes hoarseness.
- Vascular-selective lasers (KTP) can target edge vessels and reduce the risk of recurrent hemorrhage without damaging the surrounding mucosa.