
“I sound wheezy and hoarse,” complains Joe Longevity. “For the past ten to fifteen years my voice has been cutting out on me.” He adds that if he talks for long his voice squawks, then goes to a whisper for a few minutes. “Sometimes it doesn’t work at all.” Speaking is effortful. People can’t hear him in a restaurant or on the phone. A couple of years ago a doctor told him one of his vocal cords might be paralyzed. He worked on railroads for decades, on cross-country routes — a quiet job, without much talking. He rates himself a three on the talkativeness scale. Retirement has meant even less interaction, and now when he does socialize his voice is effortful, undependable, and his neck hurts afterward.
Vocal underdoers suffer from deterioration of the thyroarytenoid muscle — not from anything they did wrong, but from a lifetime of speaking less than average and, often, the added weight of age.
What Is Vocal Atrophy?
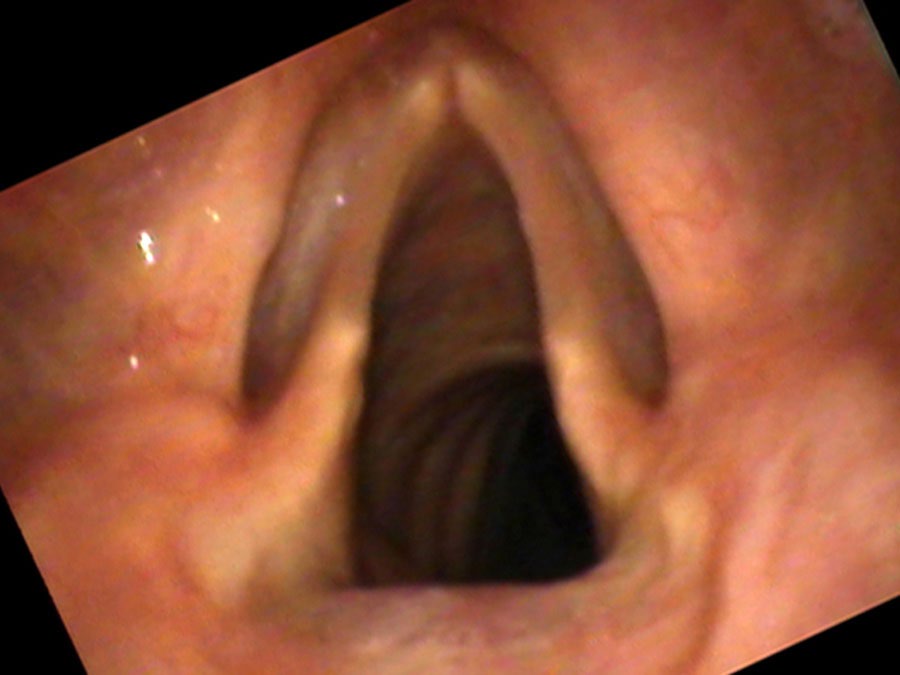
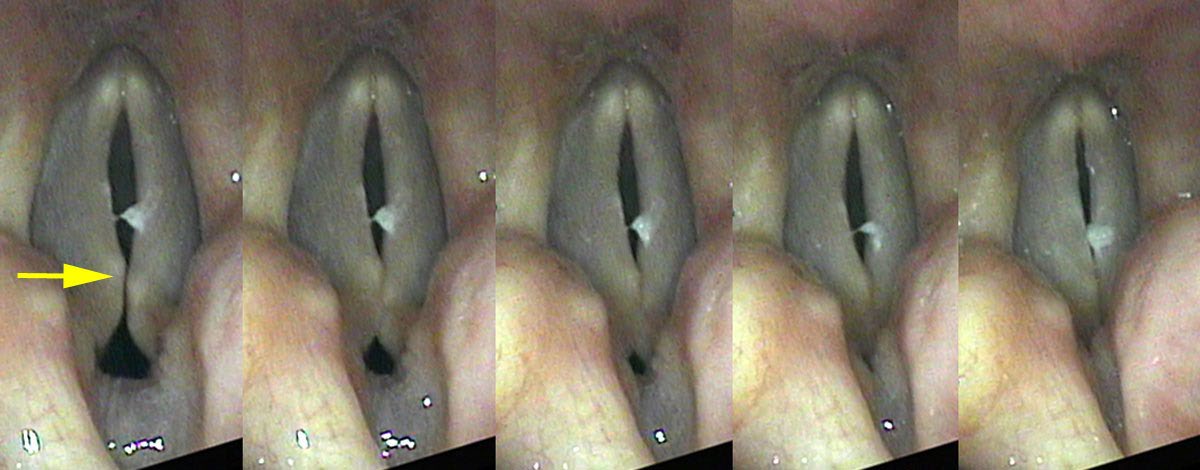
Vocal underdoers — people who rate 1, 2, or 3 on the talkativeness scale — suffer from deterioration of the thyroarytenoid (TA) muscle. The surface mucosa is fine; it is the muscle mass within the vocal cord that responds to lack of use with atrophy and loss of bulk. This is why the condition is often described as bowing — from above, the thin cords curve away from each other even when the speaker is trying to close them, leaving a characteristic spindle-shaped gap.
Ageing aggravates the problem. The elasticity of the tissues fades with age, and in a recurring cycle: as the voice deteriorates, the person withdraws from socializing, which further diminishes vocal use, which leads to further thinning of the muscle. Because bowing often occurs in older individuals it is also called presbyphonia — literally “aged voice.”
How Atrophy Sounds and Feels
With very thin cords, the vocal underdoer can position his cords for a low pitch, but without rapid air expulsion through the large gap the vocal cords fail to vibrate. The cricothyroid (CT) muscle frequently contracts to stretch the vocal cords and place them in falsetto, compensating for the large gap. Joe is obliged to use the CT muscle to make any sound at all — what is called an obligate falsetto. His speaking pitch is higher than expected for his age, nearing the female range. People on the phone assume he is a woman.
What surprises Joe’s daughter at the examination: when asked to yell, his voice sounds completely normal. “Dad, that is how your voice used to sound!” she exclaims. The yell works because explosive air pressure forces the cords together momentarily, overcoming the gap. Vocal underdoers often have not tried yelling — they are naturally not very talkative, so it simply hasn’t come up. But the preserved yell confirms the problem is not paralysis or scarring: the cords can close, they just lack the bulk to do so effortlessly at conversational volumes.
Diagnosing Atrophy on Vocal Capabilities Testing
On swelling testing at soft volumes, two findings emerge. High in the pitch range — where the CT muscle is engaged and the cords are stretched and taut — the patient can fairly easily make a soft sound without onset delays. As he progresses lower and lower in pitch, he is forced to relax the CT muscle and the bowing gap gets larger and larger. At some point he is unable to make any sound, as the air simply passes through the gap without setting the cords vibrating. The cut-off is less precise than the sharp note-specific onset delay of vocal nodules, because the gap grows progressively rather than abruptly.

Two Clinical Portraits
The Quiet Retiree
Joe’s decades of quiet railroad work followed by retirement created a long arc of vocal disuse. His cords thinned slowly and he adapted unconsciously — until socializing became so effortful and unreliable that he withdrew further still. When he yells, his voice sounds as it once did. That single observation — the preserved yell — is both diagnostic and therapeutic: it demonstrates to the patient and his family that the cords still have the potential to function well under the right conditions.
Joe decided not to undergo any procedure. He acknowledged that the problem wasn’t bothering him enough — and as a natural introvert, the prospect of having a stronger voice did not compel him the way it might have someone else. He was glad, however, to understand exactly what had happened.
The Promoted Librarian
Vocal underdoers naturally seek out occupations that allow them to be quiet — a reward for matching personality to work. Someone whose energy is drained by talking will be satisfied as a librarian or laboratory researcher, where unnecessary vocal interactions are minimized. But one day that librarian is promoted to team leader and must now run frequent meetings. Her vocal cords are underdeveloped and are suddenly called upon heavily. Like any muscle brought suddenly into use after a long rest, they fatigue easily, begin to ache, and her voice fades out with use as the muscles give out.
In summary: if a patient who is naturally quiet complains that she cannot be heard by others, or that she experiences laryngeal discomfort with required speaking, the diagnosis to search for is reduced TA muscle mass. The vocal capabilities should worsen lower in the range as compensation to close the glottic gap is progressively taken away.
Treatment Options
Treatment depends on the degree of bowing and the patient’s goals. Voice therapy can help by training the patient to use the vocal cords more assertively and efficiently — building some TA muscle mass through deliberate, intensive use. For patients who need a stronger voice for professional or social reasons, vocal cord augmentation — injecting a filler material or placing an implant alongside the vocal cord — artificially bulks up the cord so that it closes without requiring extreme compensatory effort. The patient no longer needs to squeeze as hard, the pitch drops to a more natural range, and the voice becomes effortless and reliable again.
What You Learned
- Vocal atrophy (presbyphonia) results from disuse or aging causing the thyroarytenoid muscle to thin — producing bowed cords that cannot close cleanly.
- Vocal underdoers rate 1–3 on the talkativeness scale. They seek quiet occupations and may not realize their voice is deteriorating until demands suddenly increase.
- The hallmark is obligate falsetto at conversational volumes — the CT muscle compensates for the gap — while yelling remains surprisingly normal because air pressure forces momentary closure.
- On testing, vocal capabilities worsen progressively lower in the pitch range as the TA gap grows — the opposite pattern from vocal nodules.
- Treatment ranges from voice therapy (to build TA bulk) to vocal cord augmentation (implant or injection) for patients who need reliable voice for work or social life.