
The two primary noise parameters to identify in a hoarse voice are white noise — air leak — and diplophonia, a voice with two pitches. Both can be heard and mapped on a pitch-versus-volume plot before a single endoscope is placed.
Hearing Air Leak
The two primary noise parameters to identify are white noise and diplophonia. The first question for the examiner to answer is whether the sound is clear, husky or rough — or a combination.
- Air leak is white noise generated by turbulent airflow.
- Roughness is more than one tone created by more than one sound source.
Case Study — Gabriella
Gabriella is a performer with nightly shows for another 4 weeks. She is having difficulty with her voice giving out by the end of each performance. Even while I listen to her tell me her history, I can hear a husky quality to her voice. This continues as she performs the reading task, although it can be difficult to distinguish the white noise at times with all the words and her robust volume. When she performs a maximum phonation time at her comfortable pitch, the air leak is fairly obvious. She runs out of air after 7 seconds — a very short time for anyone, much less a performer trained in vocal technique.
As she makes sounds at several pitches, working upward toward her highest pitch, I still hear air leak. Even before I get out an endoscope to look at her vocal cords, I know that the cords are not closing together completely. There is a continuous flow of air throughout much of her vocal range.
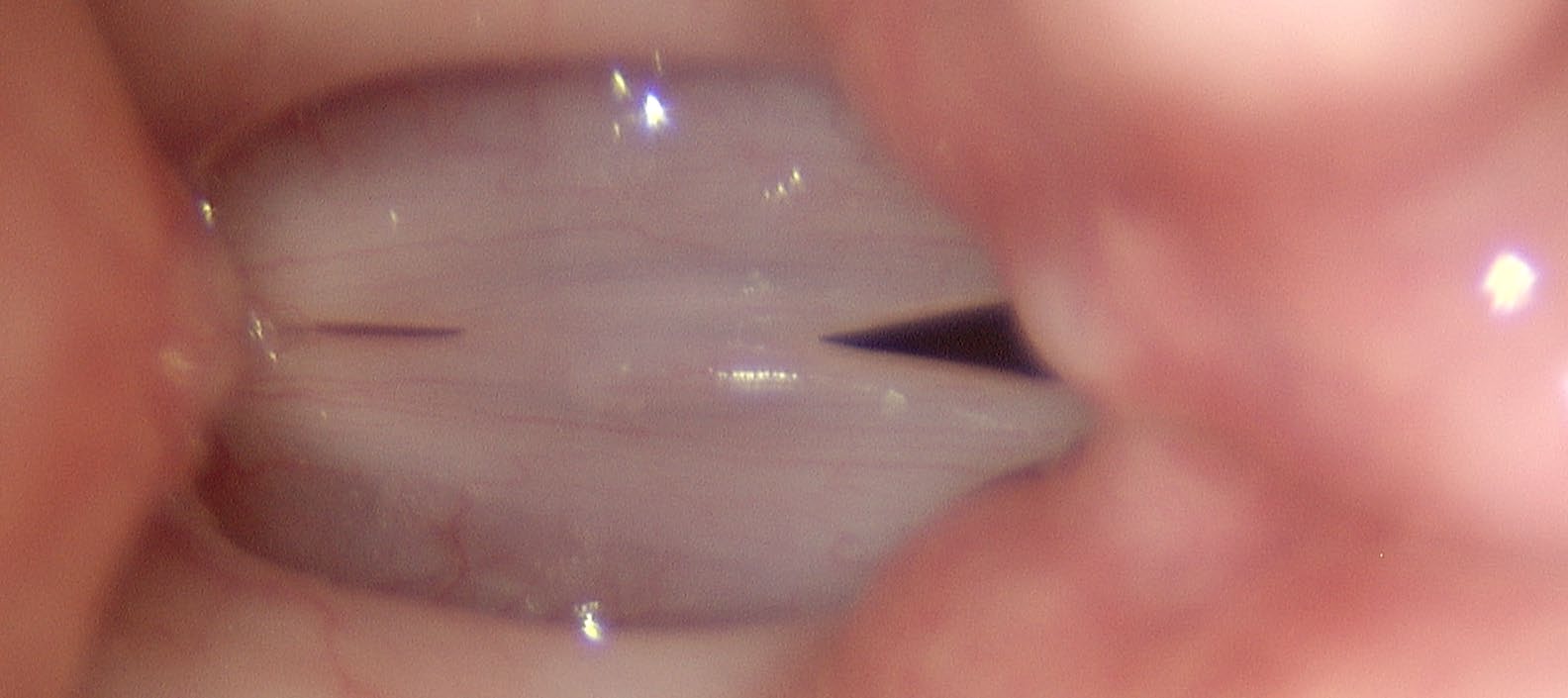
When I take a look at her vocal cords, the stroboscopic exam confirms: the vocal cords never close, even during the most closed phase of vocal cord oscillation. This particular pattern of air leak at low pitch and low volume along with air leak at high pitch and high volume is typical of large vocal swellings. The same pattern may also be typical of muscle tension, where the vocal cords are held apart by a competitive tension between the lateral cricoarytenoid muscles and the posterior cricoarytenoid muscles.
The blue areas representing air leak on our vocal diagram correspond directly to continuous dark areas during stroboscopy — regions where the vocal cords never close and turbulent air escapes as white noise.
We can — and should — test further vocal capabilities to maximally refine our differential diagnosis, and we can — and should — perform endoscopy and stroboscopy to correlate our suspected audible findings with visual findings. But at this point in the exam, we have used only vocal capabilities (reading, maximum phonation time, low and high pitch) to hear a specific vocal impairment — air leak — and already we have a strong differential.

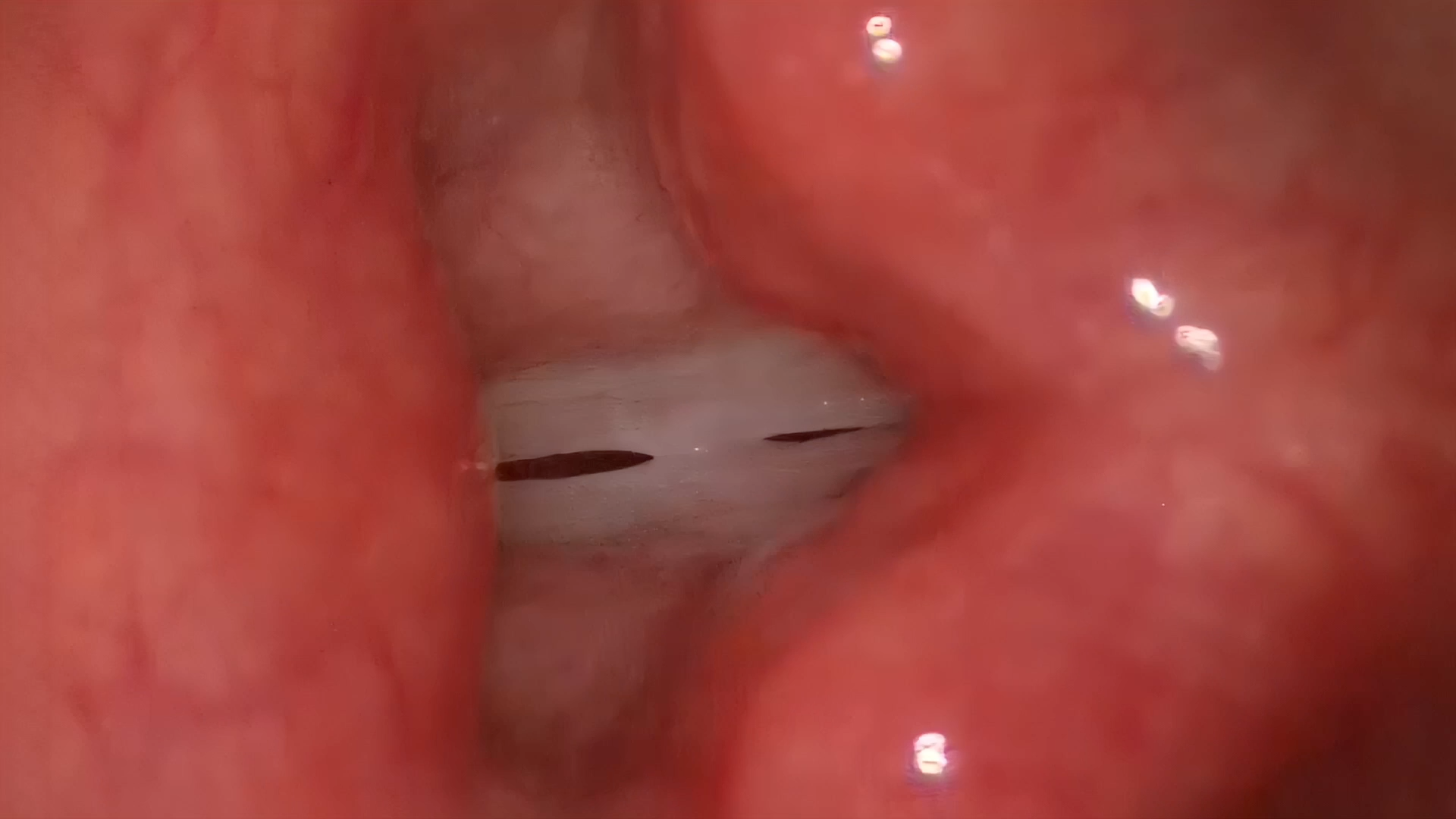
Large dark areas of air leak persist at high pitch — confirming the broad pattern of incomplete closure across Gabriella’s range.
Hearing Polyphonia
We learned that air leak corresponds to the stroboscopic finding of incomplete closure. Now we should determine what roughness — or polyphonia — corresponds to visually. Roughness in the human voice is most often diplophonia — a voice with two distinct pitches — but can be other types of polyphonia if there are more than two sound sources.
Diplophonia may be harmonic (slightly pleasing) when the two pitches are mathematically related — they will blend and augment each other to some degree. If two sound sources are not mathematically related, the sound quality will tend to be unpleasant as the two sounds interfere rather than amplify each other.
Case Study — Candy
Candy lost her voice after a cold last year. Since then, her singing voice remains rough and she cut back on singing because it makes her voice worse. In fact she recalls that for a number of years, her voice has seemed to have a “sexy quality” when she uses it too much — and she loves to talk. She rates herself a 6 on a 7-point talkativeness scale.
During vocal capabilities testing, her voice is clear and very energetic on a reading task. Her maximum phonation time at her comfortable pitch is 9 seconds — short for a singer. As she makes sounds at higher pitches, she has air leak in the middle of her range until a certain pitch, where there is a strong grating noise during phonation.
Even before I get out an endoscope, I know that something just split the vocal cords into two unequal vibrating segments. Taking a look at her vocal cords on stroboscopy confirms: the vocal cords physically touch at the pitch that generates roughness. The central swelling splits the vocal cords into two vibratory segments. The anterior segment (longer) vibrates at a lower pitch than the posterior segment. The strobe light can track only one, so the other appears to flutter irregularly.
Case Study — Nerve Paresis
A female lost her singing voice 2 years ago and when I had her glide from high to low, her voice was clear at high pitch, then alternated between diplophonic and air leak as she glided downward in pitch. She has a paresis of the left thyroarytenoid muscle. The cricothyroid muscle adds tension in her uppermost range, keeping the vocal cords relatively straight and at nearly the same tension, yielding some clarity. However, as she drops lower in pitch by relaxing the cricothyroid muscles, the left vocal cord oscillates further laterally and there is air leak. Intermittently the looser left vocal cord would oscillate at a completely different pitch from the right — producing a sound much like a flag flapping in the breeze. This is flutter: a finding occurring when there is insufficient tension on a vocal cord to maintain regular oscillations.
Two sound sources do not always generate diplophonia. Two segments of the same length — and tension and mass — will tend to vibrate at the same pitch. Even at some small difference, the sound energy from one cord may temporarily drive the other cord at the same pitch.
Summary: The Two Primary Noise Types
We have our two types of noise: air leak (white noise) and roughness (polyphonia, most often diplophonia — either harmonic or non-harmonic). The stroboscopic correlates are respectively: incomplete glottic closure where dark areas represent turbulent airflow, and two separate vibratory segments where the strobe light tracks one and the other appears to flutter. Mapping these findings on a pitch-versus-volume graph before endoscopy tells us exactly where to look and what we expect to find.
What You Learned
- Air leak equals white noise — the stroboscopic correlate is continuous dark areas where the vocal cords never fully close, producing turbulent airflow.
- Diplophonia equals two sound sources — on stroboscopy, a central swelling divides the vibratory margin into two segments, each oscillating at a different pitch.
- Air leak across all pitches and volumes suggests large swellings or muscle tension — the cords cannot close at any combination of pitch and volume.
- Flutter is insufficient tension — a vocal cord oscillating at very low, irregular pitch because one side lacks the tension to maintain regular vibration.
- MPT under 10 seconds is a red flag — especially in trained performers who should have significantly longer phonation times.