
Beyond white noise and diplophonia, the voice can be altered in its timing, pitch, stability, and silence. Each type of altered signal points to a specific mechanical or neurologic cause — and each can be heard before the endoscope is placed.
Altered Signal — Timing: Onset Delays and Pitch Breaks
Onset delays typically occur at low volumes when there is a gap between the vocal cords, or when there is a swelling that touches the opposite side and dampens easy vibration while allowing air to leak anterior and posterior to the swelling. The individual attempts to make a sound at a given pitch. Initially air leaks around the swelling and there is no sound, but then, either the individual pulls the vocal cords slightly apart or increases the subglottic pressure and the vocal cords suddenly entrain and begin oscillating, generating sound.
Pitch breaks typically occur at higher volumes when a swelling firmly touches the other side and splits the membranous vocal cord’s vibrating length suddenly into two separate segments.
Case Study — Tammy
Tammy began to notice her voice giving out while rehearsing. She is active in two different choirs and rates herself a 7 on a 7-point talkativeness scale. Her voice is clear and very energetic on a reading task. Her maximum phonation time at her comfortable pitch is 20 seconds. She has a full 3-octave vocal range. However, when I have her sing “Happy Birthday to you” at several pitches, at a soft volume, on a certain note, her sound begins as air only — then harmonic sound production starts. When she sings the same passage loudly, she does not have any audible delay. Upon returning to soft singing, the onset delay returns.
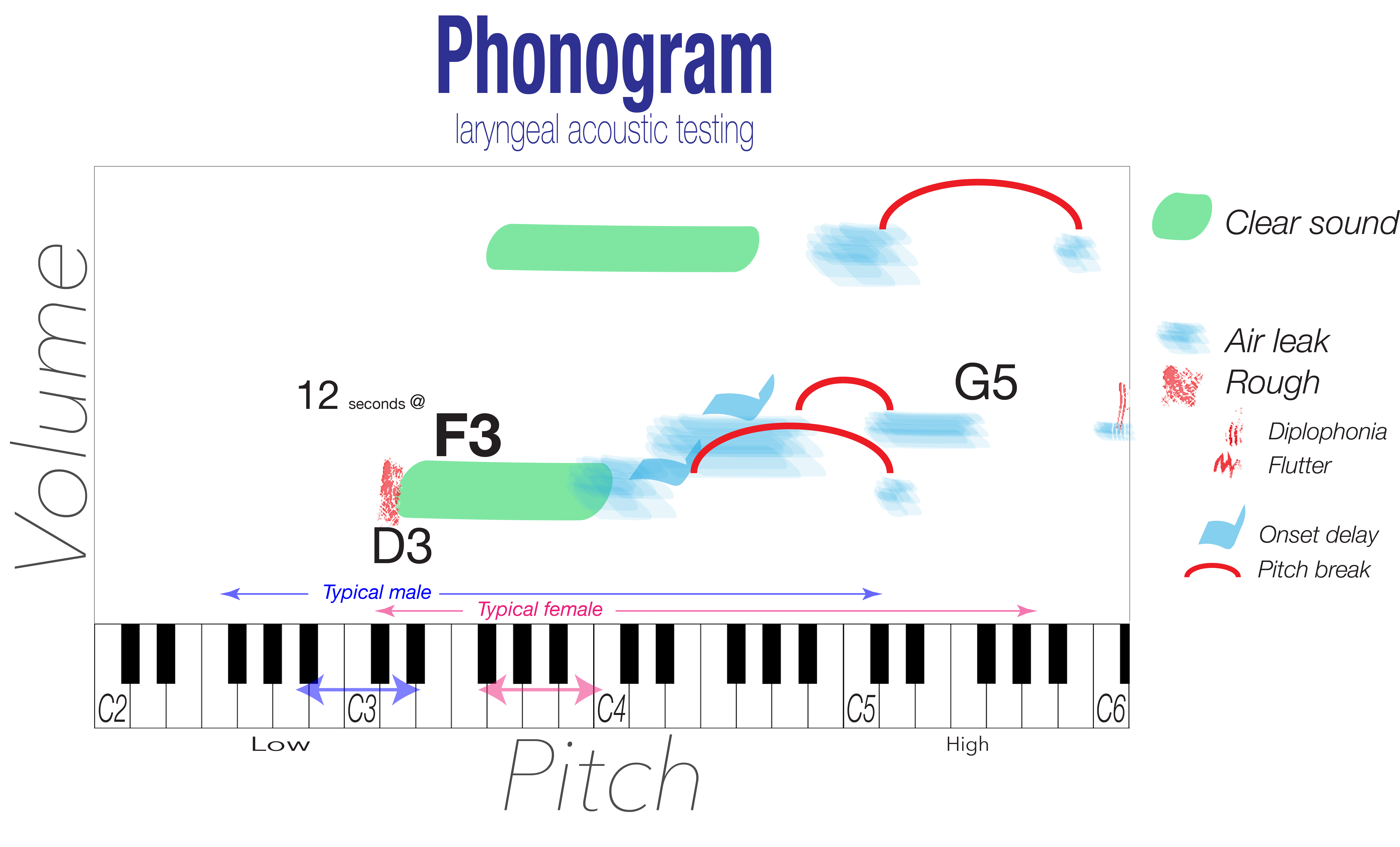
On endoscopy, I can reproduce the finding by having her glide upward at soft volume — there is a phonatory stop at approximately the same pitch. This type of impairment occurring on a fairly repeatable pitch is usually from a swelling. The onset delay represents the tension where the vocal cords are just tight enough for a swelling to touch and lightly dampen the tendency to oscillate. The reason for the delay, rather than complete aphonia, is that the individual usually rapidly adjusts — either slightly more air is passed through the cords, blowing the swellings apart, or the vocal processes are opened slightly, pulling the swellings away from each other, allowing the vocal cords to entrain.
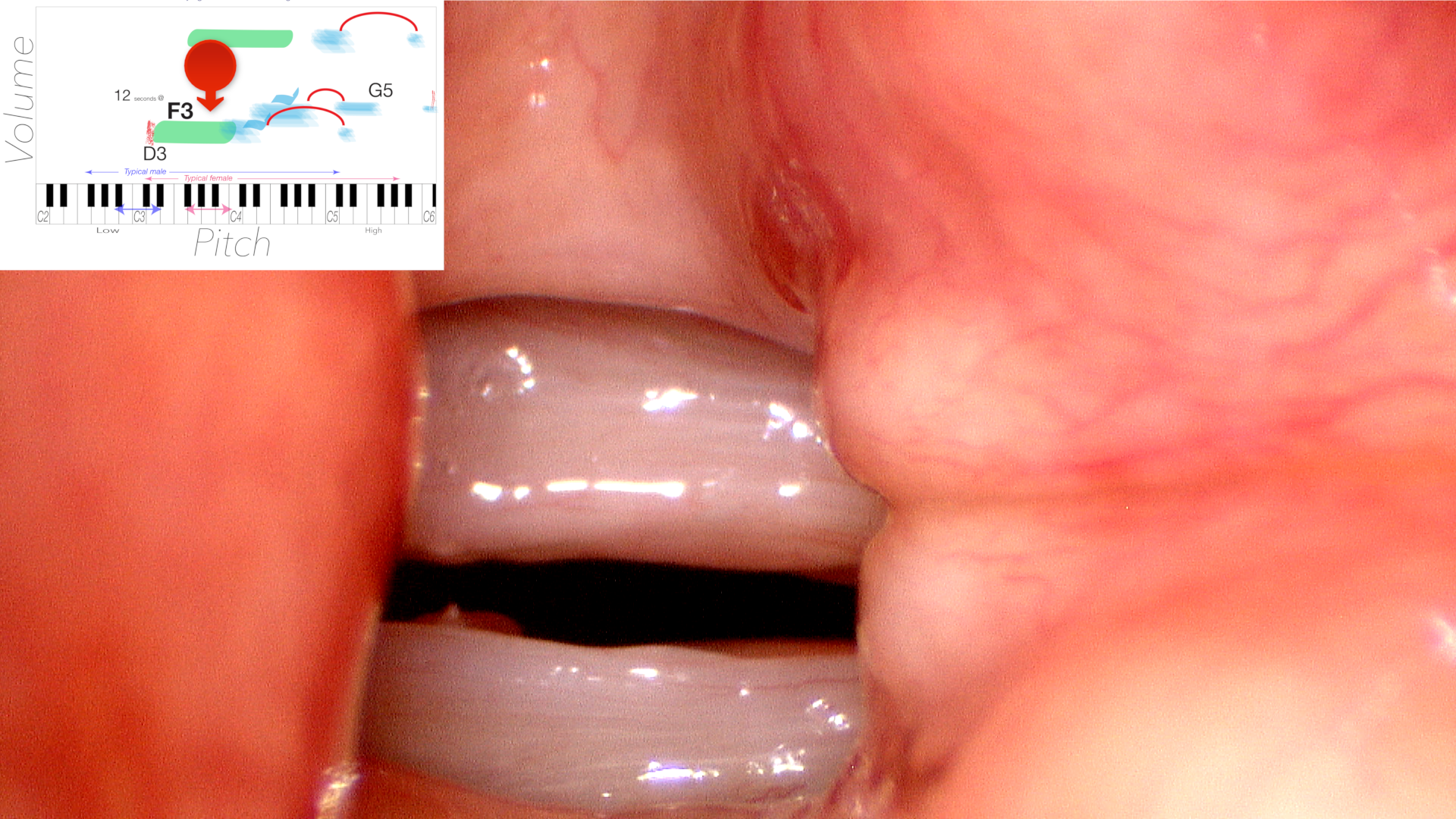

A similar mechanical phenomenon underlies a pitch break. The individual glides upward in pitch, utilizing a high subglottic pressure. When the cricothyroid muscles pull the vocal cords taut to the point where the swelling is compressed against the other side, rather than the vibrations stopping, the vibrating segment of the membranous vocal cords is suddenly split nearly in half. A vibrating structure with half the length tends to vibrate at a much higher rate — perhaps up to double — leading to a large jump in pitch, perhaps as much as an octave.
The onset delay is like putting your finger lightly on a guitar string. The pitch break is like suddenly pressing it firmly at the midpoint — the vibrating length halves and the pitch jumps.
Altered Signal — Pitch Changes
A person who cannot produce certain pitches — or who glides upward in pitch and encounters a gap in their range — likely has a structural or neurologic finding that is altering the tension, mass, or length of one or both vocal cords. Asymmetry in pitch production points to asymmetry in the vocal cord themselves. A short segment that vibrates at a different pitch from the remainder of the cord creates a very characteristic pattern on stroboscopy: a bright, active segment and a second segment that flutters or is out of phase.
Altered Signal — Stability: Tremor and Spasm
Voice production is affected by inappropriate, unstable contraction of muscles meant to be stable. This creates movement of pitch or volume and is typically under central neurologic control — termed tremor. Irregular cessation of sound production by irregular or tonic inappropriate contraction of muscles seems to be under central neurologic control and is termed spasm (or dystonia).
Case Study — Samuel (Tremor)
Samuel complains that he sounds like an old man already, and he doesn’t feel that old. During vocal capabilities testing, maximum phonation time is typically performed on a single pitch at a steady volume. Samuel’s sound alternates up and down in volume. The oscillation is regular, perhaps about 3–5 times per second. Regular instability of the sound-producing vocal cords is characteristic of a tremor. The degree of instability may vary with pitch.
Case Study — Margaret (Spasm)
Margaret complains that people are frightened of her at her new living location because of how she sounds. It is very effortful for her to speak. On vocal capabilities testing her voice intermittently cuts out during the reading task — more often on certain sounds, such as words beginning with vowels. During pitch range testing, the interruptions are more pronounced at low pitch; at high pitch, her voice sounds completely smooth. Irregular instability of the larynx is characteristic of spasm. Spasms may affect any muscle or a group of muscles, so the audible findings may vary with pitch or volume on vocal capabilities testing.
Altered Signal — Silence: Sound During Intended Silence
Generally speaking, we do not expect sound production during respiration. Recording during vocal capabilities testing may yield inadvertent sound production.
Case Study — George
George noticed that he began having trouble falling asleep about 2 years ago. When he lies down in the evening he makes sound every time he breathes inward. It has reached the point where he sits up in a chair in order to fall asleep.
During vocal capabilities testing, his voice is clear during reading, but after every phrase, he takes a deep breath and sound is produced at a higher pitch than his reading voice as he seems to struggle to get air in. This is particularly pronounced at the end of maximum phonation time testing. Even recording quiet breathing, he still makes some sound on every breath inward.
On endoscopy, his vocal cords are steady in a slightly adducted position during expiration, but during inspiration, instead of opening widely, the vocal cords adduct — and when they are close together, they entrain and produce sound during a normally quiet portion of the respiratory cycle. Whenever there is airflow and the vocal cords are close together, the Bernoulli effect will trigger entrainment and sound production.
- A fixed obstruction, such as scarring of the vocal cord joints after prolonged intubation, will produce sound both during inspiration and during expiration.
- A variable obstruction, such as respiratory dystonia or inspiratory stridor during athletics, results from active adduction during inspiration putting the vocal cords into a nearly parallel position.
- Sound may also be produced in areas of the trachea from stenosis or collapse of the tracheal airway.
Sound will be produced by the vocal cords if they are near one another and air is passed between them — no matter which direction the air is moving.
What You Learned
- Onset delays are repeatable at a specific pitch — a swelling touches the opposite cord at that pitch and momentarily dampens vibration. More variable delays suggest a gap rather than a swelling.
- Pitch breaks occur at high volume — a swelling splitting the cord into two equal-length segments causes a sudden jump of up to an octave.
- Regular oscillation of volume is tremor — 3–5 cycles per second instability is a neurologic finding under central control.
- Irregular cuts on vowels are spasm (dystonia) — affecting specific sounds, worse at low pitch, and often better at high pitch.
- Inspiratory noise reveals adduction during inhalation — the Bernoulli effect entrains partially approximated vocal cords during airflow in either direction.