
Mrs. I. Kant Breeve had her thyroid gland removed 30 years ago. She developed a hoarse voice after the surgery. Her recurrent laryngeal nerve had been injured. Stretched, cut or somehow traumatized, the nerve stopped working after the surgery and one of her vocal cords stopped moving. The cord could not move close enough to the other vocal cord to start vibrating with air flow, so she had no voice for several months. Gradually her voice improved and eventually it recovered — or more likely it seemed to recover. She had a reasonable speaking voice for 25 years. She could no longer sing nor reach high pitches, but day-to-day, her voice was adequate for work. She accepted that as recovery.
Gradually over the past several years she started having sudden episodes of her breathing being cut off. She would be speaking and suddenly she couldn’t breathe. Every otolaryngologist who looked told her she had a paralyzed vocal cord, but that she still had “plenty of room to breathe.” Several physicians told her that her episodes of difficulty breathing were from silent acid reflux and they placed her on antacids — the pills didn’t help.
Paralysis – Paresis – Synkinesis
The word paralysis means lack of mobility. It is true that her injured vocal cord does not obviously open or close with each attempted phonation and each attempted breath. There is the implicit assumption that since her vocal cord is not moving normally there is a lack of innervation — an error. The recurrent laryngeal nerve actually has such a strong propensity to regrow that even after cutting out several centimeters of the nerve, it still often grows back to the muscles in the larynx. When the nerve grows back, the major issue is not lack of nerve input, but lack of proper nerve input.
We can say that she is suffering from a laryngeal dyskinesia. A dyskinesia may be present whether or not there is any observed motion impairment, though usually there is some impairment of motion. After a nerve injury the problems that result are, to some degree, due to the degree of reinnervation, but even more due to inappropriately directed reinnervation. In the ideal world, the injured nerve would regrow back to the muscle it used to control. In the most typical severe nerve injury about half the fibers end up going to their original muscle and the other half go to the opposing muscle. Consequently, the neurologically injured vocal cord appears to be immobile — the brain tells both muscles to contract simultaneously and the net effect is that there is no motion.
That seemed to be the case with Mrs. Breeve for many years, but something definitely changed in recent years. She began having the laryngospasms that cut off her breathing entirely for a seeming eternity (when in reality it was less than a minute, but when you can’t get air, time subjectively moves slower).
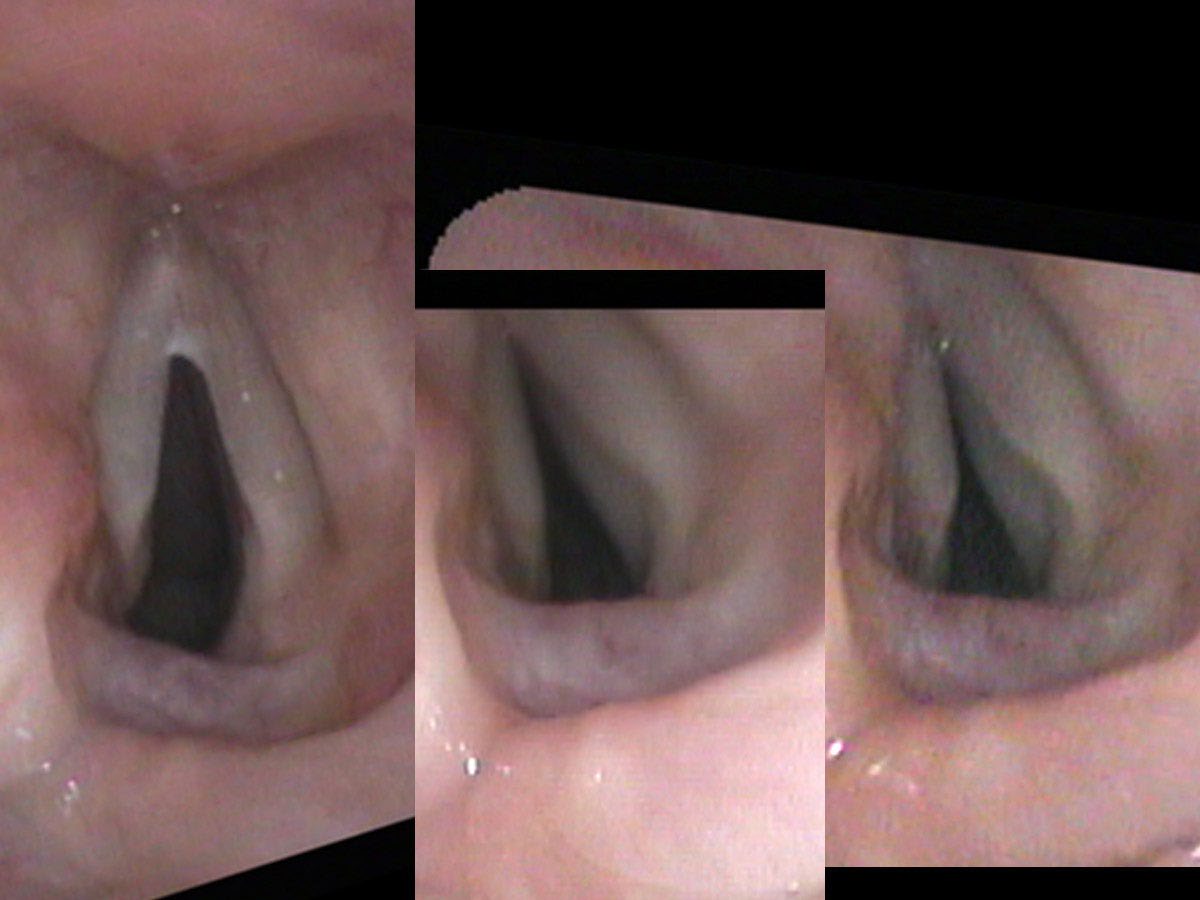
On her endoscopic exam, the healthy right vocal cord opened and closed appropriately, both during breathing and during sound production. She had quite a strong voice, though I would say that it actually had a too tight, strained quality. During the ultra-close portion of my endoscopic exam, I touched the left, non-moving or “paralyzed” cord lightly and it suddenly moved across the midline nearly closing off her airway. It wasn’t paralyzed; it could move. It just did not move intentionally and appropriately during breathing or during phonation and it was trigger-happy. With even a small trigger, her left LCA muscle would spasm and move the left vocal process nearly all the way to the opposite cord.
As both treatment and a test, I injected botulinum toxin into her dyskinetic (actually the opposite of paralyzed — hypercontracting), left vocal cord. Specifically, I put it into the TA and LCA muscles — the muscles that tense and move the cord toward the midline and closure. Two weeks later, the opening in her larynx was larger while she was breathing. She could still make sound, though a little more softly. However, she could breathe better than she had in several years and she had not had any further laryngospasms since the injection.
The paralytic effect of botulinum toxin lasted for three to four months and then the nerve regrew again and the left-sided muscles began to hypercontract again, which she could identify because of the increasing difficulty with breathing. After several injections, she asked if there was something more permanent that could be done. I suggested a surgery where we would cut the anterior branch of the RLN, then route a nerve from one of her neck muscles (the omohyoid) into the cut anterior branch supplying the TA and LCA muscles. If this new nerve sprouted fibers to the muscles before the old branch of the RLN, then she would have nerve input to these muscles during phonation — the muscles would bulk up and hold tension during phonation without tending to inadvertently spasm during breathing in.
A vocal cord’s muscles after a nerve injury are seldom really paralyzed, even if there is no obvious easily recognized movement. The vocal cord doesn’t lack movement though it may lack easily visible, intentional movement because of competing contractions. Also, it often has subtle, significant, inappropriate movement. To state it medically, after a nerve injury the vocal fold is more likely to move poorly and inappropriately (dyskinesia) than not move at all (paralysis).
It wasn’t paralyzed; it could move. It just did not move intentionally and appropriately.
Laryngospasm
Laryngospasm is the sudden closing of the vocal cords. This is a normal adaptive response to drowning. As soon as water touches the vocal cords or the lining of the trachea beneath the vocal cords, the vocal cords go into a spasm in a closed position. This stops the movement of air and prevents more water from entering the trachea and lungs. This vocal cord spasm closing off the airway typically lasts for 30 to 60 seconds before gradually opening again.
There are people like Mrs. Breeve who suffer from frequent, recurrent laryngospasm, some as often as several times per day. My experience is that laryngospasm more than once or twice a year is likely secondary to dyskinetic reinnervation after a nerve injury. Even a minor nerve injury seems to sensitize the larynx to more frequent and inappropriate laryngospasms. Whenever I see a patient with frequent laryngospasms, I look for evidence of a nerve injury.
Bilateral Vocal Cord Paresis
Mrs. Abigail Gris awoke from her neck surgery with a weak voice. Her surgeon said, “Try not to worry, this happens sometimes. The breathing tube in your throat may have caused a little swelling. Just wait, it will get better.” Over the next several weeks, her voice started to recover and in several months it seemed to be back to normal. She and her physicians assumed this was the end of her story.
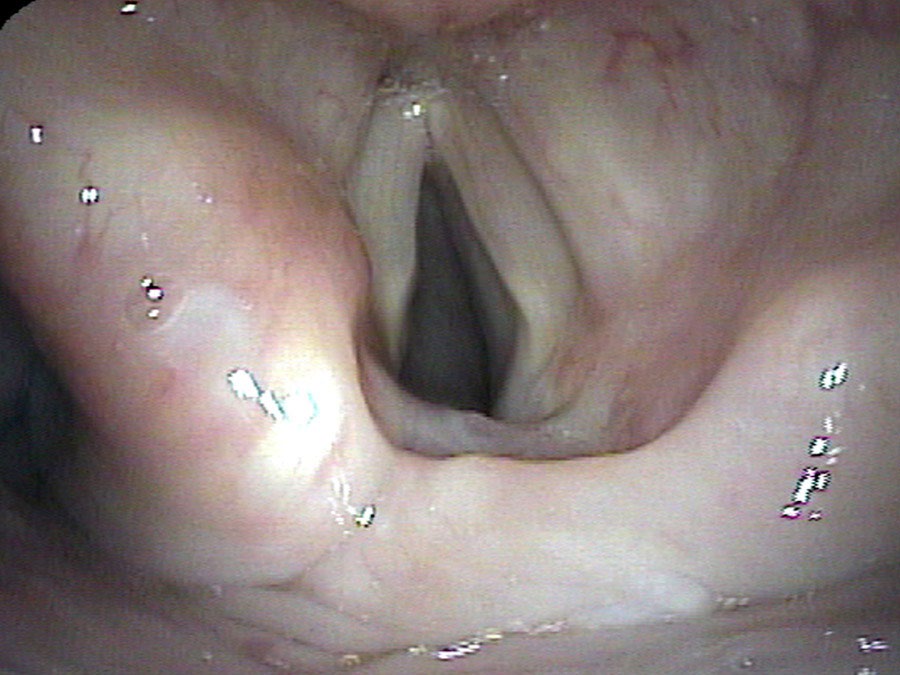
Mrs. A. Gris did just fine for five years. She again developed pain in her neck and found a new neurosurgeon who chose to approach the neck from the opposite side. Perhaps he heard her good voice and assumed that her vocal cords were working normally. She awoke from this second neck surgery with no voice again. Over a few weeks her voice started to return, but it was still weak when I first saw her. The right vocal cord, previously injured, was seen to be in a nearly fixed position near the midline. The left vocal cord, newly injured, could move slightly apart with breathing in.
Unfortunately, the regrowth of the injured RLN, while very helpful in a one-sided injury, usually becomes a significant problem when the same regrowth happens on the second side. Over the next several months, her voice did indeed become stronger as the nerve grew back. Breathing also became more difficult. When she would actively breathe in, the recently injured left cord would actively close. Enough of the fibers that normally opened her vocal cords during inspiration (via the PCA muscle) had grown into the muscle that closes the vocal cords for speaking (LCA muscle) such that, the deeper she breathed in, the more strongly the left cord closed.
Her options had become very limited. A tracheostomy — a hole in the neck with a plastic or metal tube — allows breathing through the neck bypassing the vocal cords. A one-way valve can be placed so that air enters through the tube but is directed out through the vocal cords for generating sound on expiration. There are other options such as permanently cutting or partially removing one of the vocal cords, or removing the arytenoid cartilage (arytenoidectomy) to enlarge the airway. However, the larger the opening into the windpipe, the softer the voice becomes, and the more that liquids and food go down the wrong way — increasing pneumonia risk.
There are no good choices, just bad ones with a lot of compromises. If you have ever had an RLN injury, before considering any additional surgery on your neck or chest, you should have a good laryngeal exam to assess the risk. Even with a normal voice, it is possible to have one vocal cord that does not move well or at all. Operating near the already injured nerve is a small risk. Operating near and injuring the nerve on the opposite side ends up as a significant, life-altering event.
What you learned
- After a nerve injury, the RLN regrows strongly but indiscriminately — fibers often cross to opposing muscles, producing a “paralyzed-appearing” cord that is actually hypercontracting (dyskinesia), not silent.
- Frequent laryngospasm (more than once or twice a year) is a red flag for dyskinetic reinnervation after a prior nerve injury — the cord is trigger-happy, not truly still.
- Botulinum toxin injected into the hypercontracting muscles can relieve laryngospasm and improve breathing; a denervation-reinnervation (DeRe) surgery can make this more permanent.
- Bilateral RLN injury is a catastrophic and life-altering event — a strong reason to obtain a thorough laryngeal exam before any second neck or chest surgery, even when the voice sounds normal.
- The correct term for most post-injury vocal cord conditions is dyskinesia (inappropriate motion), not paralysis (no motion) — the distinction drives the treatment.