
Barbara S. Ma has been hoarse for several months. She appears a bit older than her age, with the fine facial wrinkles of someone who has smoked tobacco for some time. She attributes her current problem to her husband, who several months ago began smoking again. Although he had stopped for a year, he resumed smoking after a stressful occasion at work. Barbara is a former smoker and says that her hoarseness came on about a week after her husband resumed smoking. She is concerned that she may be developing cancer, both because of her former smoking and her husband’s current second-hand smoke.
When I review her various medical diagnoses, I note that she checked off the asthma box, yet she is not on any medication for it. I inquire about her asthma and she says, “Sorry, I forgot, I am also on an inhaler. I am using Advair™ (fluticasone/salmeterol), but my asthma is under excellent control.” She had been switched to Advair about 4 months before her hoarseness started.
Looking, But Not Seeing
When I place the endoscope through her nose and begin to view her larynx, the larynx appears with a reddish hue. This is the view obtained by the typical otolaryngologist who examines the vocal cords from five or more centimeters away. Many physicians tend to focus on the back of the larynx and state that the “interarytenoid area is red, so it must be reflux.” Since I have never seen reflux laryngitis, I move the endoscope extremely close to her vocal cords.
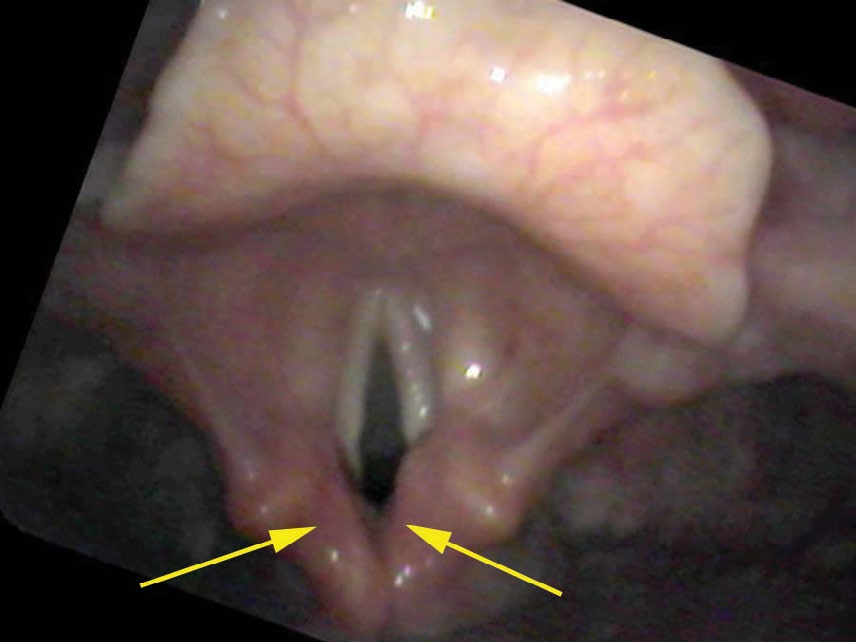
From a distance, there are always a couple of illusions present. The throat appears red because the mucosa covering the throat is translucent — you can see through it. The red or pink color comes from the vessels beneath the mucosa. Moving closer, when mucosa is seen straight on, it is only lightly pink as the blood vessels are spread out. Yet when viewed in a plane nearly parallel to the endoscope, mucosa appears redder, because while you still see through the transparent mucosa, in an angled or parallel view, all of the vessels end up being stacked on one another, so visually there is more apparent redness.
Diagnosis and Treatment
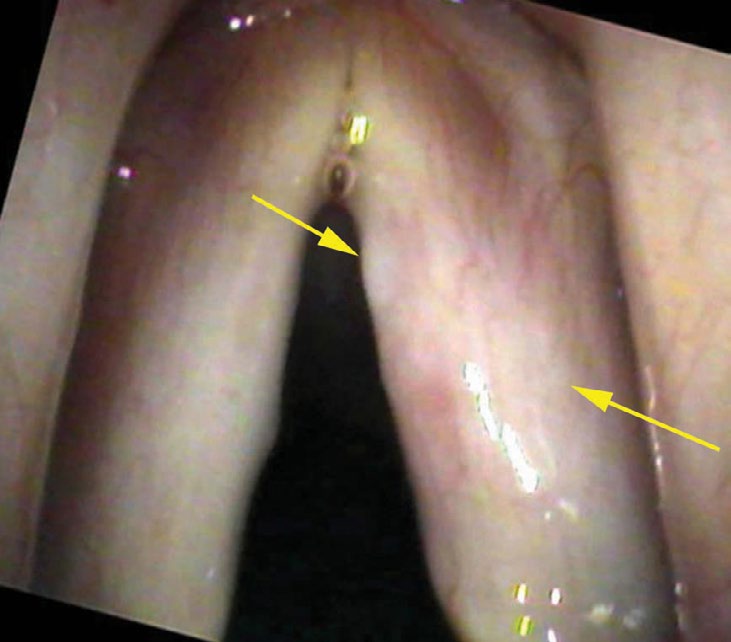
If we stop and search this close-up view for a time, we will begin to perceive that all of the vessels dim in the central portion of the vocal cord. They are actually diving under a thin film of white. Because the vocal cord itself is white, a white film on the surface (white on white) is not easily discernible. But if we concentrate on the vessels, we can see a distinct curving line where the vessels fade or disappear as they traverse the central portion of the vocal cord.
I make a diagnosis of fungal laryngitis since I perceive a whiteness and the typical throat fungus is Candida albicans, which is white. Fungus growing on the vocal cords would also stimulate increased blood flow or inflammation. The patient is on a steroid spray that, while very good for the prevention of asthma, will encourage the overgrowth of the normal fungal flora in the mouth and throat (also known as thrush).
I treat her with four weeks of fluconazole and teach her how to rinse her vocal cords off after each use of the Advair inhaler. Typically when one gargles, all the water is in the back of the mouth since we naturally try to keep water away from the vocal cords. To bypass this tendency, a patient places a curved cannula in the back of their throat and while saying “eeeeeeee” drips water directly onto the vocal cords. Because air is coming up while saying a sound, the water bubbles on the surface of the vocal cords and a laryngeal gargle is created.

A Lesion That Resembles Cancer
There are more blatant examples of fungal infections. A suppressed immune system from treatments such as chemotherapy or systemic steroids for a prolonged period can lead to bright white, fuzzy patches growing all over the larynx and even the rest of the throat. I have also seen a few patients on steroid inhalers where the layers of fungus build up to the point that the lesion resembles a cancer.

Within three to four weeks of treatment with an antifungal the lesion disappears. I reassured Mrs. Ma that although her husband’s smoking was not healthy, it was not the cause of her hoarseness and she did not have a vocal cord cancer. I utilize her video recording frequently in my lectures to alert physicians that they may be taking pictures of the problem and looking at the problem without ever really seeing the problem.
The goal is not to see a color. The goal is to see what is stiffening the vocal cords — in this case, the film of white fungus and the surrounding edema from a surface infection.
What You Learned
- Fungal laryngitis — typically from Candida albicans — is a common and underrecognized complication of inhaled steroid use (Advair, Flovent, and similar medications).
- Apparent redness of the larynx viewed from a distance is largely an optical illusion: the mucosa is translucent and angled surfaces appear redder because capillaries are stacked visually. Redness alone is not a diagnosis.
- The key finding is a thin white film on the surface of the vocal cords that partially obscures the blood vessels beneath — visible only on very close inspection, often within one millimeter of the cord.
- The voice is rough because the fungal film stiffens each cord asymmetrically, causing them to vibrate at different pitches.
- Treatment: four weeks of an antifungal (fluconazole) plus a laryngeal gargle after each inhaler use to remove deposited steroid.
- In immunosuppressed patients, fungal deposits can be extensive enough to mimic cancer — but they resolve completely with antifungal treatment.