
When the history and the laryngoscopy don’t fit the common diagnoses, unusual organisms must be considered. Two patients illustrate this principle: one with valley fever on the vocal cord, and one whose persistent hoarseness had been dismissed as reflux for more than a year before tuberculosis on the vocal cord was discovered.
Valley Fever — Coccidiomycosis
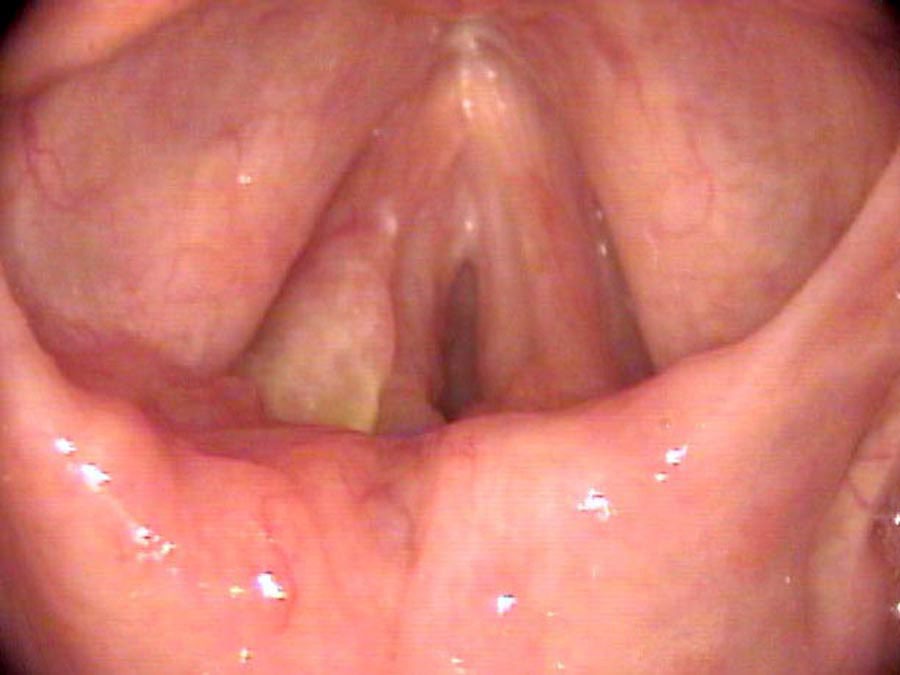
Jesus Juarez had difficulty breathing starting three months ago. He thought it was just a cold but it progressed. In the emergency room he was given epinephrine and steroids to help his breathing. When asked about prior problems, he recalls that 20 years ago he was hoarse for a year while living in central California. He had nodules on his vocal cords that when biopsied, he was told that he had “Valley Fever” or coccidiomycosis.
On his close endoscopic examination there was a bulbous collection of giant cells growing out of the left arytenoid area. When something with an unusual shape or form is growing on the larynx, a biopsy is a very appropriate next step. The office biopsy revealed coccidiomycosis had invaded his larynx and was preventing his vocal cords from opening well.
Tuberculosis
Moon Lee moved to the United States five years ago. Last autumn, he returned to Korea for a conference and developed a cough that persisted on his return. By December, he had lost much of his upper singing voice and was persistently hoarse even when speaking. He could not project his voice anymore. An ENT told him that he had reflux laryngitis and recommended that he avoid spicy foods.
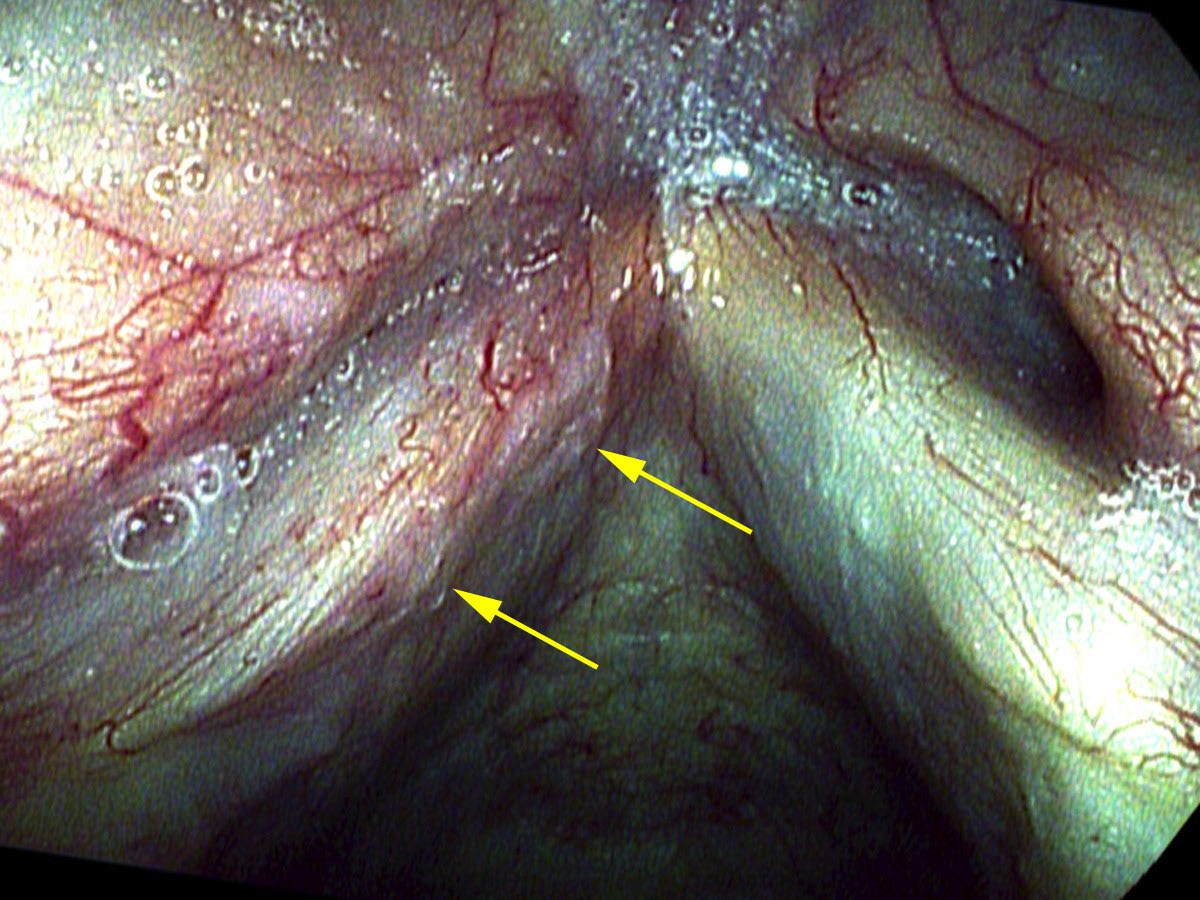
On my endoscopic examination, there were irregular swellings on the edge of the left vocal cord. This was my first view of tuberculosis on the vocal cords. There were cells of Mycobacterium tuberculosis in his sputum when cultured. He was referred to an infectious disease colleague and received extended treatment for tuberculosis.
When something with an unusual shape or form is growing on the larynx, a biopsy is the appropriate next step. A diagnosis of reflux laryngitis should never be made without close laryngoscopic examination.
What You Learned
- Unusual organisms — fungi such as Coccidioides immitis (valley fever) and mycobacteria such as Mycobacterium tuberculosis — can infect the larynx and cause progressive hoarseness and airway compromise.
- A prior history of the same organism (even decades earlier) raises the possibility of reactivation and is an important diagnostic clue.
- Coccidiomycosis on the larynx produces a bulbous, giant-cell collection with an unusual shape — very different from the common vocal cord lesions and requiring biopsy for diagnosis.
- Tuberculosis on the vocal cord produces irregular swellings along the cord margin and may be mistaken for other lesions or dismissed as reflux without close examination.
- Any unusual or undiagnosed growth on the larynx warrants biopsy. Geographic history and travel history are essential parts of the laryngology workup.