
Verna Solo is almost 80. She noted the onset of hoarseness for three months but another problem took precedence. Her aorta had been enlarging for several years and her cardiac surgeon felt that she needed surgery to repair her dilated aorta last month. She woke up from surgery with only a whisper. While her voice has returned, it remains very raspy.
In thinking about possible reasons for her hoarseness, one consideration is that she could have a weak voice because the dilating aorta stretched her recurrent laryngeal nerve, causing a nerve injury. So perhaps her progressive hoarseness before the surgery and the enlarging blood vessel are related. Her weak voice immediately after a surgery near the recurrent laryngeal nerve suggests that a nerve injury during surgery is a possibility to be considered as well, and we might find a paralyzed vocal cord during endoscopy. We also know that endotracheal tubes in the throat can cause an injury and weakness after surgery.
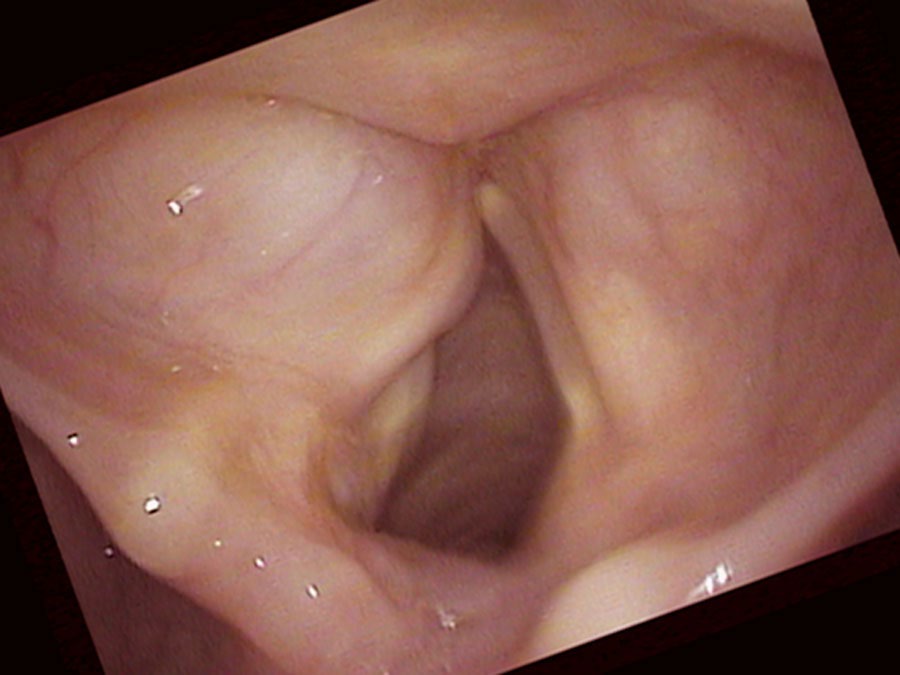
Indeed, I find one of these possible explanations when I look with the endoscope: her left vocal cord is not moving well. It is not opening and closing very much during breathing nor during voicing. However, it does sit near the midline. Sorting out her case requires thinking about a few complexities. She can almost close the right vocal cord against the left, so she has already compensated quite a bit for the paralysis.
I ultimately numb her vocal cords so that I can place my endoscope underneath the smooth, round, swollen left false vocal cord. The left false vocal cord is dilated and obscures the left true vocal cord. There is a fluid-filled cyst enlarging the left false vocal cord. The left vocal cord is also not moving and in the view during inspiration, the left vocal cord remains positioned near the midline. Even on a close-up view it is difficult to see the left true vocal cord. I actually have to lift the swollen false vocal cord up with the endoscope to see the true vocal cord.
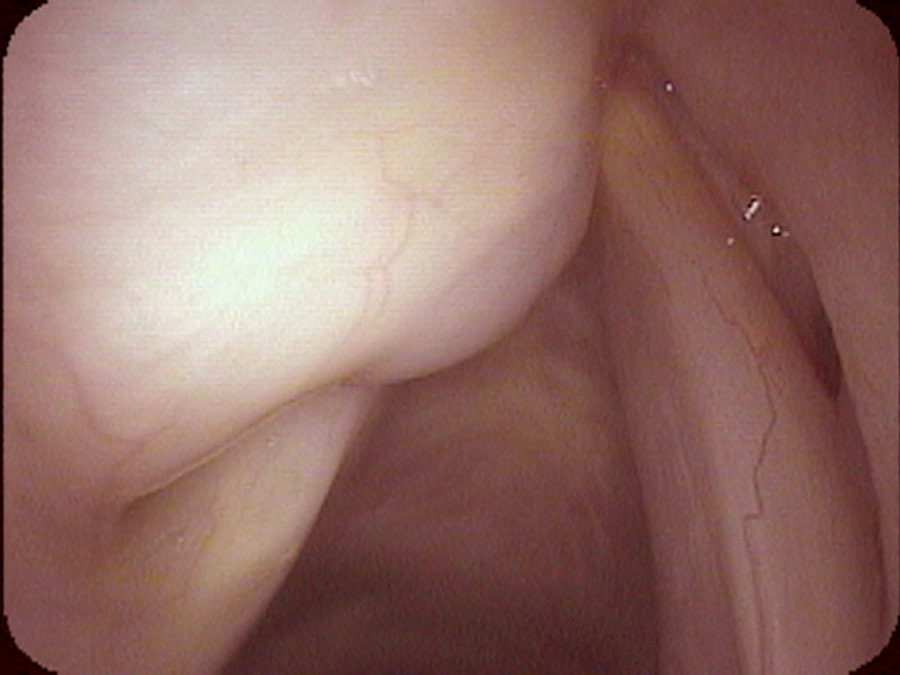
The saccule is a gland located on the bottom of the false vocal cord at the front of the larynx. Usually the saccule cannot be seen from above. However, occasionally this gland may plug and fluid accumulates inside it. The saccule swells with its own fluid creating a saccular cyst. Now we must consider that we have a complex problem: a left vocal cord that is not completely paralyzed — it moves some. So there is synkinesis of the left vocal cord. The right vocal cord closure has compensated to the point that she can bring the two vocal cords together. Consequently, even though the left cord’s neurologic injury is visually obvious, since the right vocal cord closes against the left during sound production, they are not causing air leak (husky hoarseness). Since the left cord has reinnervated, it also has the same bulk as the right vocal cord and so it is not causing diplophonia (rough hoarseness).
As an examiner, it is sometimes possible to become so focused on finding an expected problem that something large and in the field of view may be missed. The striking visible abnormality is not always the actual cause of the patient’s complaint.
I anesthetize her vocal cords and put the endoscope almost on the vocal cords and watch them vibrate when she makes sound. The left-sided saccule has enlarged to the point that it pushes down on the true vocal cords. This pressure on the vocal cords dampens their vibrations. It then requires more air or effort to start and to keep the vocal cords vibrating. Her saccular cyst is actually causing her vocal effort and her weak voice — by rubbing on both vocal cords when she tries to make a sound. Even though she has an obvious left-sided vocal cord movement impairment, it is only a striking visible abnormality and not actually the cause of her weak voice.
In the end, as Mrs. Solo lived alone, she decided not to have a biopsy, an excision or anything done surgically to improve her voice. When a person comes in with a complaint of, “I am hoarse,” this should not be interpreted as, “Please find all the abnormalities in my throat and fix them,” but rather, “Please find the problem that is causing my hoarseness, tell me what can be done about it and what are the risks.” In the context of hoarseness, this means that we must find the gap or the asymmetry or both depending on what type of hoarseness they have.
What you learned
- A single patient can have multiple simultaneous laryngeal disorders — in Verna Solo’s case: a left vocal cord paresis with synkinesis, and a left saccular cyst pressing on both true vocal cords.
- Synkinesis occurs when a reinnervated vocal cord regains bulk and midline position even though its movement is abnormal — making it look better than it really functions.
- When the right vocal cord has compensated by closing across the midline to meet the left, there may be no air leak and no diplophonia — even with an obvious paresis — because the actual cause of hoarseness is something else entirely.
- A striking visual finding (like a paralyzed vocal cord) can distract the examiner from the true cause of the patient’s complaint — the false vocal cord must always be examined carefully, including lifting it aside if needed.
- The goal of the consultation is not to find and fix every abnormality, but to identify which abnormality is actually causing the patient’s specific complaint and to discuss the risks and benefits of treatment.