
Mrs. Seeka Tris comes in with her daughter Susan for a second opinion. They really like their doctor, and don’t want him to know that they are seeing me, but it has been such a rough time that Susan thought it might be worthwhile. “Mom had mitral valve surgery last spring. When she woke up after the surgery, things didn’t go very well. She ended up in the ICU for 10 days with a tube in her throat on a ventilator. She recovered, and we’re happy, but when the tube came out she couldn’t speak except for a whisper.”
Mrs. Tris went home with a soft voice. Over about a month, her surgeon’s prediction proved correct and her voice began to recover. By two months, she was speaking much better, almost with a normal volume. However, her breathing worsened enough one night that she called her daughter. At the emergency room, a ventilation-perfusion scan ruled out pulmonary embolus and she was sent home. She visited a pulmonologist (breathing tests, bronchoscopy), then an ENT (“vocal cords not working well”), then a laryngologist (bilateral vocal cord paralysis, confirmed by EMG), then a neurolaryngologist (botulinum toxin injection to one vocal cord to open the airway). Six months after waking without a voice, the injection has made her breathing a little worse rather than better. She is now in my office for another opinion.
With a history of voice loss after a tube in the throat, there are two likely reasons. First: if the cuff of the endotracheal tube was inflated too much and too close to the undersurface of the vocal cords, it may have put pressure on the nerves entering the vocal cord muscles — causing a nerve injury. Second: the hard plastic tube may have put pressure on the cartilages between the vocal cords at the back of the larynx. Even in as little as two hours, this pressure may injure the mucosa. After the tube is removed, the ulcerated area contracts and scars over several weeks, pulling the back of the vocal cords together.
In a nerve injury, the vocal cords will not be moving well after the tube is removed. However, the recurrent laryngeal nerve has a very strong propensity to regrow — over a few weeks to a few months the nerve sprouts new endings that grow back to the muscles. Several months later, the voice may become strong again, but the vocal cords may fail to open during breathing. Mrs. Tris’s pattern — improving voice, then worsening breathing — fits this picture.
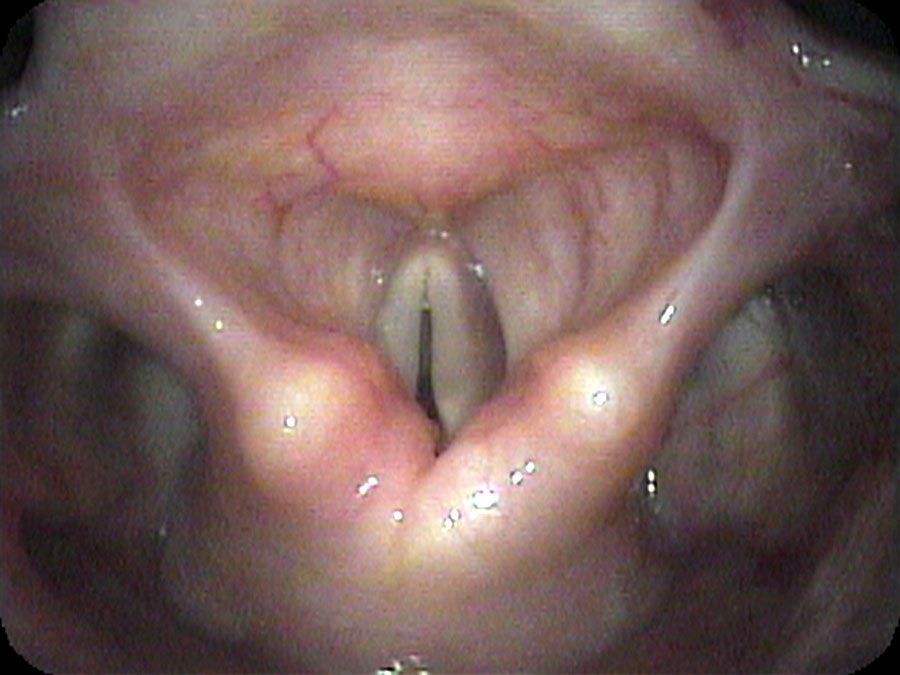
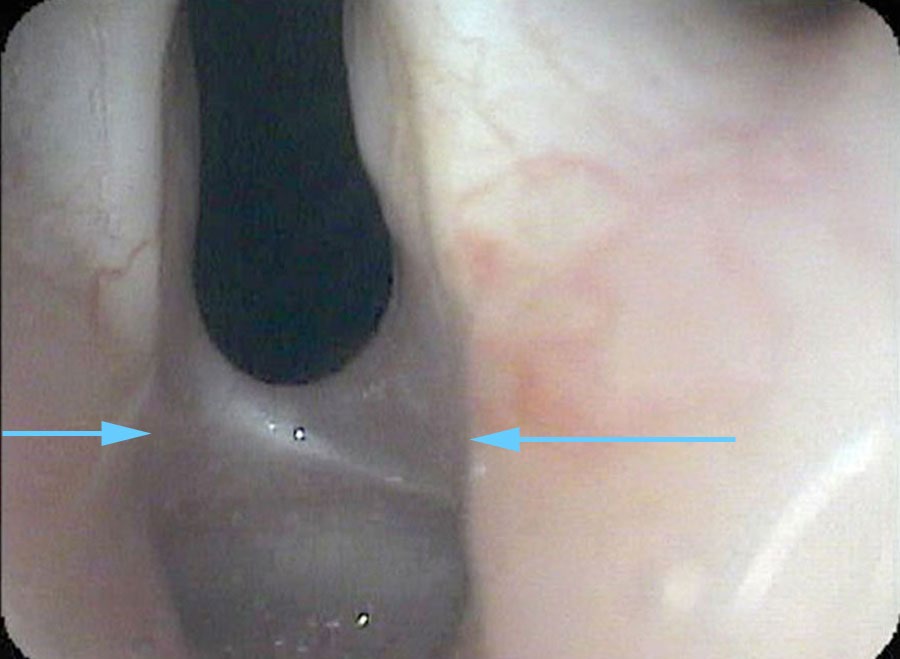
I drip some numbing medication onto her vocal cords and pass the endoscope under the arytenoids at the back of the larynx — looking at the area where the endotracheal tube would have been sitting for 10 days. I find a band of scar tissue just beneath the vocal cords, holding the vocal cords together. At most, she can open her vocal cords about 2 millimeters because of this scar band.
When you visit a doctor about a problem, don’t ask yourself, “How much is this going to cost?” What you really want to know is, “How much value will I receive for this advice?”
I think back on the cost of Mrs. Tris’s diagnosis: the emergency room visits, the tests, the procedures, the consults, and not the least, the amount of time it took from her life for her to get the correct diagnosis. It is quite possible to go in with surgery to divide this scar tissue — but only if you know what the problem is. The longer the delay, the more likely the joints will have become fixed in one position, reducing the chance of full restoration.
Interestingly, our body functions like a well-engineered system, and problems with the system are generally quite understandable in scientific or engineering terms. If a physician has the luxury of good endoscopes and a recording system, the physician should not only be able to diagnose a problem, but should be able to explain to the patient why it is not working — and the patient should be able to see this. The explanation should make sense to anyone. If the explanation a doctor offers seems mystical or mysterious in any way, there is a high probability that it is a contrived explanation.
What you learned
- A scar band (posterior glottic stenosis) from prolonged intubation is mechanically distinct from vocal cord paralysis — but both produce similar-appearing immobility on a standard endoscopic overview.
- Passing the endoscope beneath the arytenoids and very close to the posterior commissure is the only way to directly visualize a scar band in this location.
- Botulinum toxin injection to reduce abductor muscle activity worsens breathing in posterior glottic stenosis — the opposite of what would be expected in bilateral paralysis — making the diagnostic error clinically consequential.
- The value of a precise diagnosis is measured not just in cost avoided but in time returned: six months and multiple procedures could have been compressed into a single close-proximity endoscopic examination.
- An explanation of a voice or breathing disorder should always make sense in mechanical terms. If it doesn’t, the patient is right to ask for a clearer answer — or seek one elsewhere.