
The thyroarytenoid (TA) muscle lies within and runs the length of the membranous vocal cord. It provides most of the filling or mass of the vocal cord, and it is the primary muscle for controlling pitch in the chest register.
The larynx is comprised of 10 muscles — five on each side. With the various muscles changing the position, length, and tension of the vocal cords, quite a range of sounds can be generated. Since each muscle is paired, any asymmetric contraction represents a probable weakness. Understanding the function of each muscle will help one understand neurologic and muscular injuries especially well.
During phonation at a low pitch, the vocal cords are brought together but tension remains relatively loose, leaving the vocal cords short and thick. At high pitch they are conversely tight, long, and thin. The muscles are hidden from our direct view, though in some cases we can see the bulk of the muscle beneath the surface.
The TA Muscle
The TA muscle lies within and runs the length of the membranous vocal cord. The muscle provides most of the filling or mass of the vocal cord. It tightens to increase the pitch, mostly by isometrically tensioning the vocal cord. For singers when they are not engaging the CT muscles, the TA muscle essentially is used to change pitch throughout their lower or chest register.
The TA muscle provides most of the filling or mass of the vocal cord — and is the primary pitch-control muscle in the chest register.
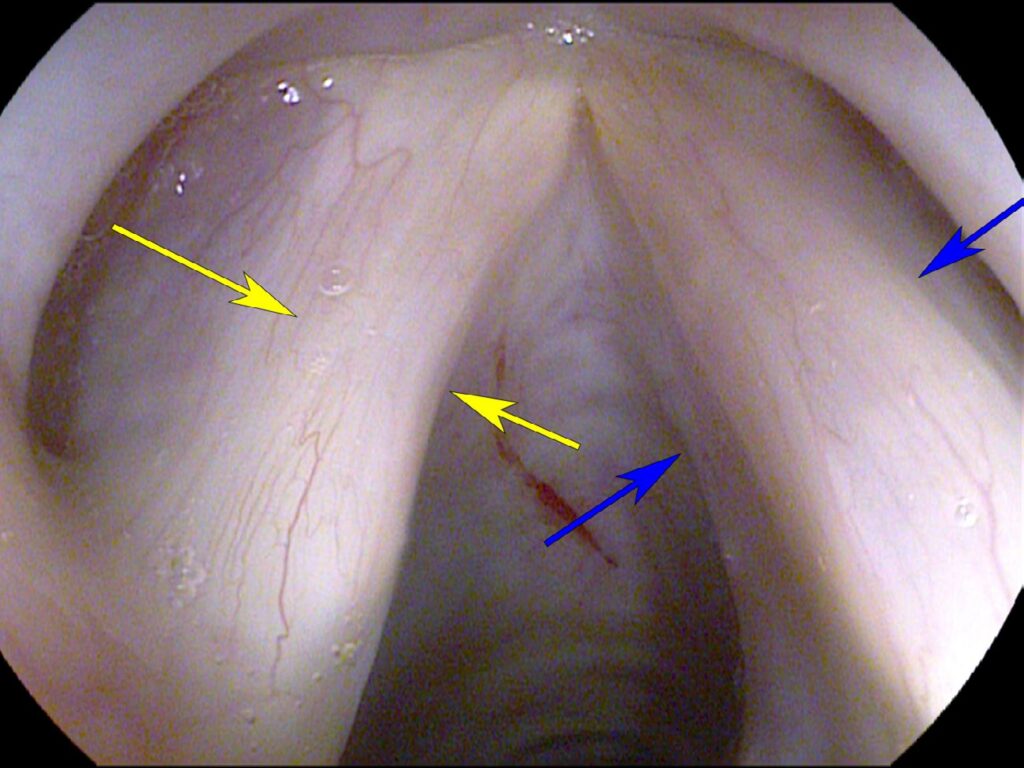
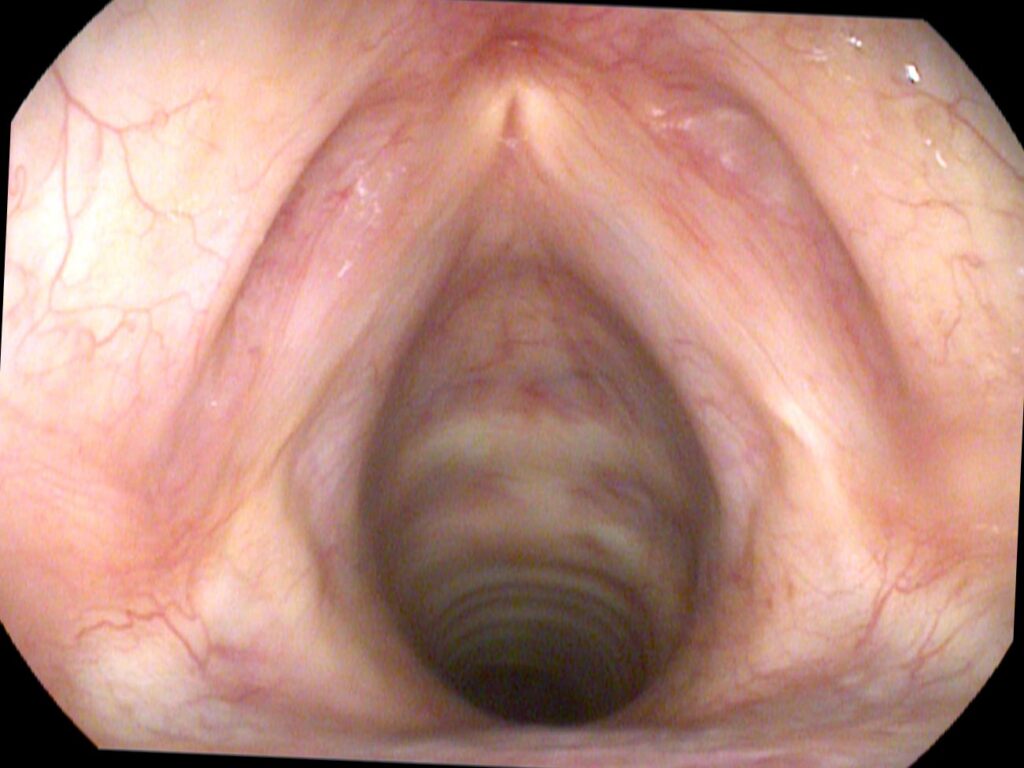
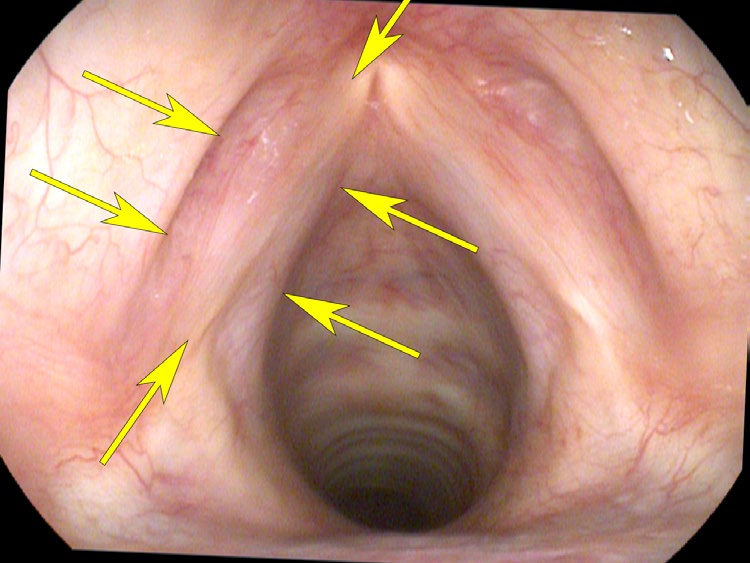
We can see the bulk of this muscle during endoscopy on a healthy vocal cord. The easiest way to appreciate the bulk is in the patient where one vocal cord is completely paralyzed, especially when viewed along the length of the vocal cord. In a complete paralysis, the paralyzed vocal cord would consist of only the mass of the vocal ligament. The difference in size between these vocal cords then represents the mass of the thyroarytenoid muscle.
What You Learned
- The TA muscle is the vocal cord’s primary mass — it fills the membranous cord and provides the bulk visible on endoscopy.
- It tightens isometrically to raise pitch, making it the dominant pitch-control muscle in the chest (lower) register.
- Atrophy is visible — when one side is paralyzed, the size difference between the two cords directly shows how much of the cord’s bulk comes from the TA muscle.
- Each muscle is paired — asymmetric contraction or size difference is a reliable sign of unilateral weakness or neurologic injury.