During the office visit, I want my attention focused on hearing the patient’s story. I not only want the details about when, where and how the vocal impairment seemed to start, but I want to hear this story from the patient directly.
- The telling of the story gives me a sense of the patient’s priorities in terms of solving the problem.
- I am also actually hearing the problem as they use their voice to tell me the story.
- I get a sense of the patient’s preexisting biases that I may need to deal with later in the exam.
One of the areas I find very useful is what the patient recalls from seeing each physician before me. Even if I have the actual physician’s notes of the prior appointment, I still want to hear what the patient recalls. I will then know if I need to address some preexisting bias. For example, many times during a history a patient tells me that he is hoarse because of GERD. He just has not improved on treatment directed at GERD, so he believes he just hasn’t had sufficient treatment. Even if I don’t believe GERD has anything to do with his hoarseness, at the end of my exam I need to not only tell the patient about my recommended treatment, but I also need to address his belief in GERD as a cause of his problem.
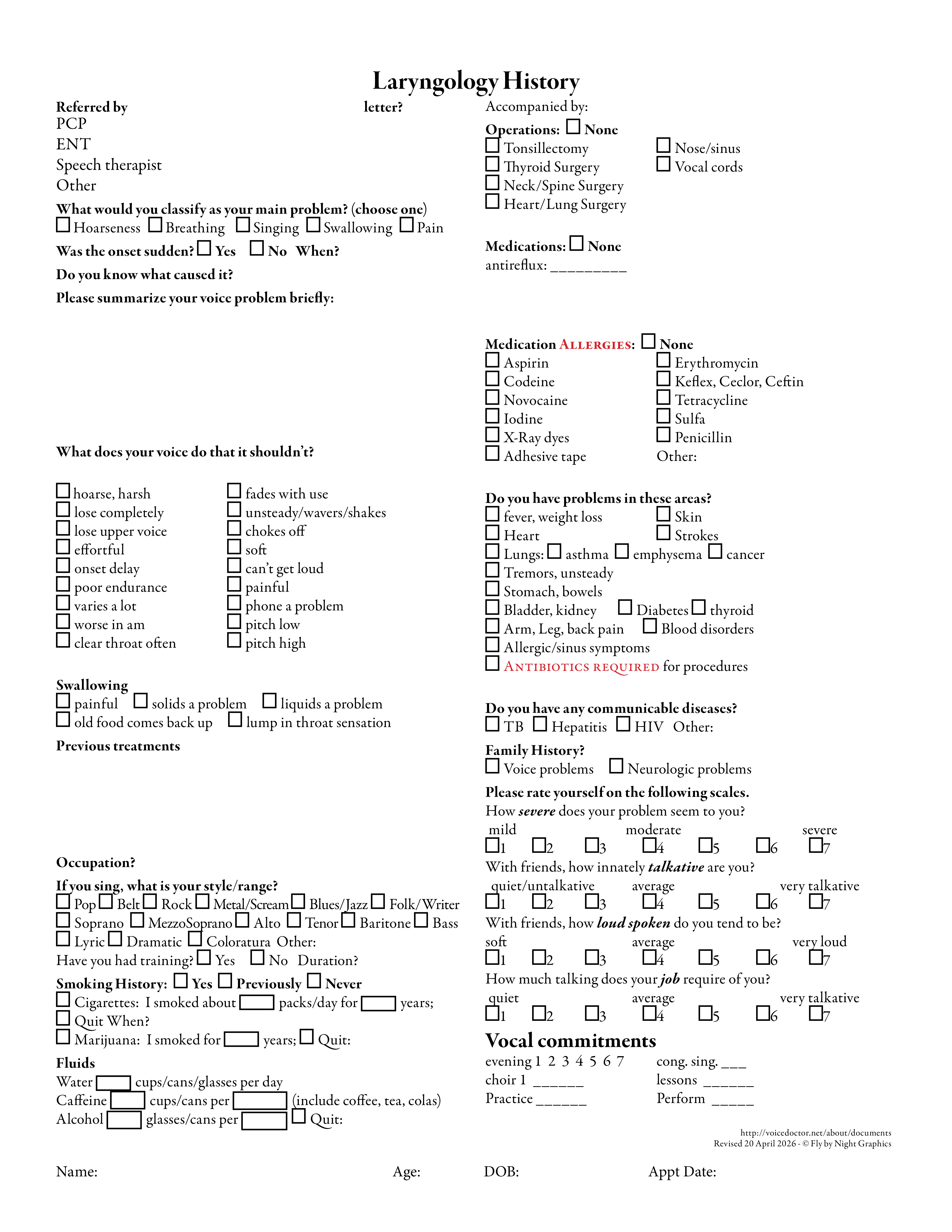
A medical history is fairly standardized across medical specialties. I designed an intake form to collect details relevant to hoarseness before I visit with the patient. This form covers talkativeness, loudness and work vocal use — three areas that may not be in a typical otolaryngology intake form. I assess how much time the individual devotes to singing, the full ENT overview of the head and neck region, and the patient’s own perception of the severity of their problem.