
It is the difference between looking and seeing. Even with the most expensive equipment, if the examiner does not maneuver the endoscope to the appropriate location, the result can be a zero-definition examination — missing the pathology completely.
From Snapshot to High Definition
It seems simple to put a camera in the nose or mouth and look at the larynx. Indeed, that is what many examiners do. It is simple. And with a simple approach, the examiner ends up with basically a snapshot.
If John purchases a professional SLR camera and sets it on program mode, aims and pushes the shutter button, he still ends up with photos that look like snapshots. Meanwhile, Sarah, a professional photographer with an eye for light and emotion, can capture scenes with an iPhone that look spectacular. Of course, with a professional camera, Sarah can do much more. She knows how to use the tool in her hand. The same is true for the laryngologist.
A high-definition exam uses techniques to put the pathology onto more pixels than a colleague does — with even the same equipment. Even if the camera on your endoscope has 1 million pixels, if you do not maneuver the endoscope to the appropriate location, you can essentially end up with a zero-definition examination.
Recording — Audio and Video Together
Any recording of the larynx is better than the human eye looking into an endoscope. Too much happens, and it happens too quickly, for the human eye to perceive much of it. Digitally recording directly is probably the easiest method.
Three recording practices significantly improve quality: immediately upon completing a recording, review the video on a high-resolution monitor — this quick review can be done while preparing to explain findings to the patient, and it gives the examiner an opportunity to resume endoscopy if a finding is not completely clear. Perform a secondary review later when selecting still images for a written report — looking frame by frame often reveals findings initially not perceived during the examination. And maintain a searchable database with parameters recorded for each exam — when encountering a laryngeal finding that is new, looking up previous exams for comparison is invaluable.
The Standard Complete Exam
There are several valuable features of performing the same standard, complete examination in most patients. Even if areas of anatomy and function seem not seemingly relevant to the current patient’s complaint, by recording the same complete exam in each patient, the examiner is less likely to miss something, has a record for the future when a different issue becomes retrospectively relevant, makes thousands of observations that teach him what normal anatomy and function look like — making atypical findings more recognizable — and learns to record slowly and deliberately.
On a live exam, it seems like forever watching someone take a breath, but when reviewing video, three breaths may not be enough to fully evaluate respiratory motion. Three seconds of phonation during stroboscopic recording at a given pitch may only give you a single cycle of vocal cord oscillation that is fully in focus. You will wish you had recorded more.
Assessing Palate and Pharynx
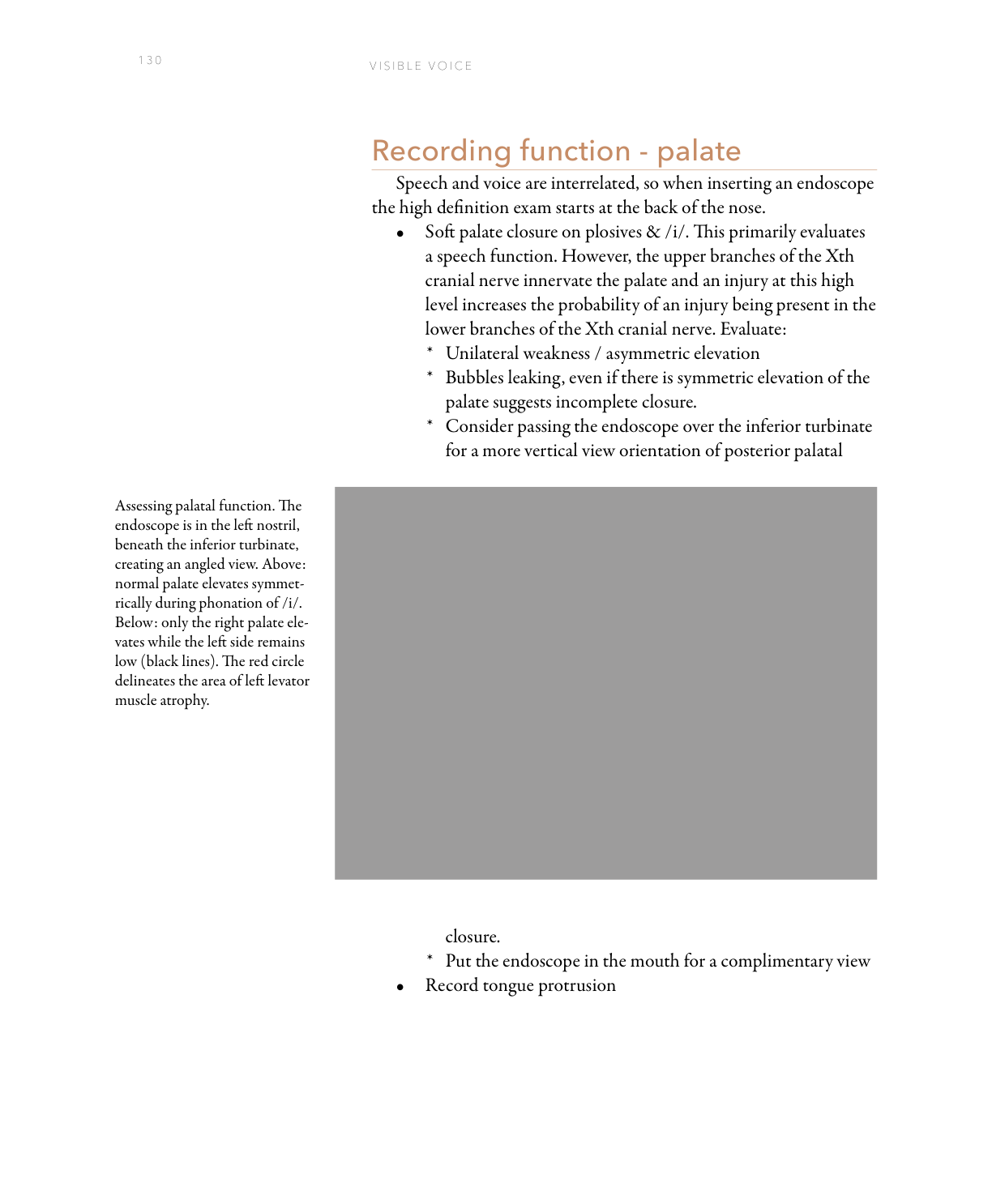
A high-definition exam starts at the back of the nose. Soft palate closure on plosives and /i/ primarily evaluates a speech function. However, the upper branches of the Xth cranial nerve innervate the palate, and an injury at this high level increases the probability of an injury being present in the lower branches of the Xth cranial nerve — including the recurrent laryngeal nerve. Observe for unilateral weakness, asymmetric elevation, or bubbles leaking past the palate despite seemingly symmetric elevation.
Pharyngeal constriction and symmetry during high-pitch phonation reveals the activity of the pharyngeal constrictors. A vocal glide from a high pitch to a low pitch will show the vertical muscular thickening of the pharyngeal constrictors on each side. Watch for any lateral deviation of the posterior pharyngeal median raphe at high pitch — and keep the endoscope high in the pharynx because the larynx will rise suddenly with attempted high pitch.
Assessing Laryngeal Function
Observation of vocal cord planar motion — abduction and adduction — during quiet respiration reveals a natural, moderate abduction during inspiration and a partial adduction during expiration. During sniffing, maximal abduction is easily visualized. Direct attention to timing of adduction and abduction:
- In paralysis, the injured side does not move.
- In paresis, the injured side moves appropriately through a reduced range.
- In synkinesis, the injured side may be static (as in paralysis) but will hold tension during phonation and have thyroarytenoid mass on close examination.
- In dyskinesis, the injured side may move in an inappropriate direction and/or at an inappropriate time of the respiratory cycle.
- In hyperdyskinesis, the injured side may hyper-adduct during sniffing, after phonation or after other stimulation — and may be adducted past the midline in a state of tonic contraction.

Stroboscopy and Closeness
When the complaint is hoarseness, the goal of the examiner during stroboscopy is to explain white noise and diplophonia. Examine vocal cord oscillatory motion at several pitches, directed by abnormal findings during vocal capabilities testing. Look for gaps (anterior, posterior, central), asymmetry (neurologic, stiffness), and the number of sound sources (side-to-side or anterior-to-posterior).
The most powerful technical upgrade is closeness. Every bit closer makes a greater than expected increase in the magnification of the image. The closer an endoscope is to the reflected light, the brighter the image. The closer the chip to the pathology, the more pixels filled by the disorder and the higher the effective resolution. At extreme closeness, capillary architecture is near microscopic levels with higher-definition chip endoscopes. Topical lidocaine allows touching of the vocal cords for extreme close-up views.
The examiner with a flexible endoscope who moves the scope closer to the vocal cords overcomes the three deficits substantially: the image is clearer, brighter, and has less digital artifact.
Selective Color Imaging
Colors are selectively filtered to increase the contrast between red and other colors — this becomes more valuable with increasing resolution. Capillary orientation is very characteristic in tumors and papilloma:
- Normal capillaries tend to be small, similar in diameter, and parallel to the vibratory margin of the vocal cord.
- Scar capillaries tend to be perpendicular to the vocal cord vibratory margin, varying a bit more in diameter.
- Post-radiation capillaries appear frond-like, almost like patches of ferns, and are larger than normal. They form over months to two years after external beam radiation.
- Papilloma capillaries form smooth loops running perpendicular to the surface mucosa and may appear as dots when viewed directly from above.
- Dysplastic and carcinoma capillaries are oriented perpendicular to the surface mucosa, irregular, often multilobulated, with greatly enlarged feeding vessels surrounding them.
Companies have tended to trademark the software algorithms they use for selective color imaging. Olympus calls their software narrow band imaging (NBI). KayPentax calls theirs iScan.
What You Learned
- Technique matters more than equipment — a skilled examiner with modest equipment will outperform an unskilled examiner with a top-tier instrument.
- Closeness is the highest-impact upgrade — more magnification, more light, less electronic noise, all in one maneuver that costs nothing.
- Electronic gain creates red artifacts — a generally red-appearing larynx is often an artifact of the camera’s auto-gain compensating for the endoscope being too far away.
- Palate evaluation begins the neurologic exam — CN X branch injury at the top level raises the probability of injury in the lower branches supplying the larynx.
- Selective color imaging maps capillary architecture — distinguishing normal, scar, post-radiation, papilloma, and malignant vessel patterns can achieve an “optical biopsy” in the office.